Severe tricuspid regurgitation (TR) can have a poor long-term prognosis.1 Given that its isolated surgical treatment has been associated with increased mortality,1 the need for minimally invasive techniques has prompted the development of the percutaneous treatment of this valve. In recent years, several percutaneous techniques have been proposed for the correction of TR. Although little evidence is available, implantation of the MitraClip system (Abbott Vascular, Santa Clara, United States) in the tricuspid position appears to be the most commonly-used technique at present.2 In this article, we present the first case of percutaneous tricuspid repair performed in Spain.
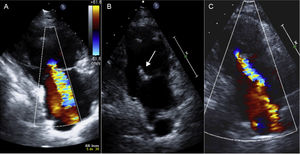
The intervention was performed in a 65-year-old woman with symptomatic severe primary TR (extreme fatigue and lower limb edema), with right ventricular dilatation but no pulmonary hypertension. Transesophageal echocardiography (TEE) showed severe TR with a central jet, probably secondary to restriction of the septal leaflet (Figure 1), but with an anatomy favorable for clip implantation, as leaflet length was > 10mm, with adequate thickness and no areas of calcification. Because surgery was contraindicated due to morbid obesity, we decided to perform a percutaneous repair with MitraClip. The technical details of the procedure have been described previously,3 but, briefly, 2 clips were implanted between the anterior and septal leaflets, as after release of the first clip we observed a partial detachment of the septal leaflet, which was stabilized with the effective implantation of a second clip in a more central position (Figure 2). The patient was discharged at 48hours with a transthoracic echocardiogram (TTE) that showed a reduction in TR from grade 4/4 to grade 2/4.
. C: 2/4 TR at 2 months postprocedure. TR, tricuspid regurgitation.")
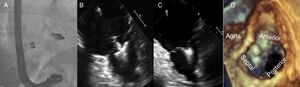
 and septal (right) leaflets. D: 3D-TEE image showing the final position of the second clip between the anterior and septal leaflets. 2D, 2-dimensional; 3D, 3-dimensional; TEE, transesophageal echocardiography.")
Fluoroscopy image sequence and TEE during the procedure. A: final position of the clips on fluoroscopy. B and C: 2D-TEE image at 0° with the clip open and closed after the attachment of the anterior (left) and septal (right) leaflets. D: 3D-TEE image showing the final position of the second clip between the anterior and septal leaflets. 2D, 2-dimensional; 3D, 3-dimensional; TEE, transesophageal echocardiography.
At follow-up at 4 months postimplantation, the patient reported clear symptomatic improvement. Follow-up TTE demonstrated the stability of the result at discharge, with grade 2/4 residual TR, and normalization of the right ventricular diameters and a mean tricuspid gradient of 2mmHg (Figure 1).
In recent years, percutaneous intervention on the cardiac valves has undergone rapid growth.4 While interventional treatment of the aortic, pulmonary and mitral valves has the advantage of more available clinical evidence, interventional treatment of the tricuspid valve is still in a very early phase. With various degrees of success, numerous conceptually distinct techniques have been proposed, such as percutaneous implantation of an aortic valve on top of degenerative tricuspid prostheses, percutaneous annuloplasty devices, and even balloon-type devices with the aim of occupying space in the valve and thus reducing the regurgitant orifice.1 However, despite the scarcity of the available evidence, MitraClip appears to be the most frequently-used system with the largest number of presented cases to date.1,2 The largest series published so far is that of Nickenig et al.2 which had 64 patients. In that series, 1 clip was implanted in 48% of patients and 2 to 4 clips were implanted in 42%. In 78% of the patients, the clip was positioned between the anterior and septal leaflets. In addition, in 97% of patients, at least 1 clip could be implanted, in 91% TR was reduced by at least 1 grade, and no periprocedural deaths were recorded.
After reviewing the literature and presenting our impressions after this first implantation, we believe that the use of MitraClip in the tricuspid position has 3 inherent challenges: a) the use of a system that can only attach 2 leaflets in a valve with 3 leaflets (anterior, posterior and septal); in this regard, after studying several ex vivo models, we concluded that the attachment of the anterior and septal leaflets appears to be the combination that is associated with greatest reduction in TR2,4; as is the case with the mitral valve, the intervention also aims not to induce moderate or severe valve stenosis (mean gradient > 3mmHg); b) the second is the tricuspid approach of a 24-Fr system designed to be directed at the mitral valve; although right femoral access is the most frequently-used, transjugular access has been proposed, which, despite being awkward for the operator and the difficulty of controlling hemostasis after the procedure, permits direct access to the valve2; and c) imaging assessment of the tricuspid valve with 2-dimensional/3-dimensional (2D/3D) TTE/TEE is another of the major challenges of this technique: the need to learn and obtain planes that allow good visualization of the valve anatomy and provide a reliable guide during the procedure is a crucial element in the development of this technique.
In conclusion, the use of MitraClip in the tricuspid position appears to have promising results, but new registries need to be published to determine whether the treatment is safe and effective in the long-term.
CONFLICTS OF INTERESTM. Hernández-Enríquez has received a training grant in interventional cardiology from the Spanish Society of Cardiology. X. Freixa and M. Sitges are proctors for Abbot Medical.
.