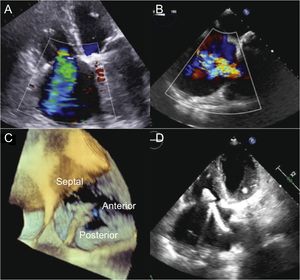
A 71-year-old woman was admitted to our hospital for right-sided heart failure (HF). The patient had a history of rheumatic disease and 2 surgical interventions. In 1976, she underwent open mitral commissurotomy, and in 2003 she underwent mitral valve replacement with a mechanical prosthesis and De Vega annuloplasty of the tricuspid valve. During follow-up, symptoms and signs of right HF appeared, and echocardiographic studies documented normal functioning of the mitral prosthesis with severe tricuspid regurgitation (TR) due to restriction of the tricuspid valve leaflets (Figure 1A). She was given medical treatment, but after an initial response period, the clinical picture recurred with severe limitation of quality of life. The multidisciplinary team decided that she was at very high risk for conventional surgery, but offered her the possibility of a MitraClip implant in the tricuspid position to treat her advanced HF symptoms. Prior to the procedure, transesophageal echocardiography (TEE) was performed, confirming the severity of TR and that the tricuspid leaflets were adequate for device implantation (Figure 1B). The catheterization procedure showed only mild pulmonary hypertension and the absence of coronary lesions.

Screening echocardiography and procedure. A and B, TTE and TEE show severe RT. C, positioning and orientation of the clip in 3-dimensional TEE to capture the anterior and septal veils. D, grasping in TTE. TEE, transesophageal echocardiography; TTE, transthoracic echocardiography; TR, tricuspid regurgitation.
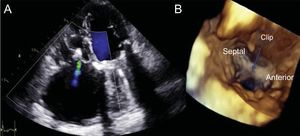
The procedure was performed under general anesthesia and was guided by TEE. The guide catheter was advanced through the femoral vein and was positioned in the lower area of the right atrium. The clip was introduced into the guide catheter using the Munich technique and was then advanced into the atrium to the straddling position. Subsequently, it was deflected toward the tricuspid valve using wheel A and was guided to capture the anterior and septal leaflets. However, as the clip was advanced into the ventricle to capture the leaflets, we could not achieve an adequate visualization of the clip arms using the acoustic shadow of the mitral prosthesis. To achieve sufficient image quality, we switched to transthoracic echocardiography, and finally grasp was achieved with a significant reduction in TR to grade mild-moderate (Figure 1C-D). After confirmation of adequate leaflet insertion and the tricuspid gradient (1 mmHg), the clip was released. Postprocedural control echocardiography showed that the clip was in position with a double-orifice tricuspid valve and residual mild-moderate TR (Figure 2A-B).

Functional TR comprises more than 90% of cases of TR and is mainly due to annular dilatation and right ventricular growth secondary to left-sided heart disease.1 Patients with TR and secondary HF are often highly symptomatic because of decreased cardiac output and peripheral and abdominal congestion. In addition, the presence of moderate or severe TR is associated with high mortality, regardless of biventricular function and pulmonary pressures.2 Current data support tricuspid repair at the time of surgical intervention on the left heart; however, reintervention for persistent or recurrent TR is associated with high morbidity and mortality.3,4 Likewise, a significant proportion of patients are left with recurrent TR following tricuspid repair surgery, particularly after De Vega or Peri-Guard annuloplasty.4 In these cases, transcatheter tricuspid repair techniques have emerged as an alternative to conventional surgery.1 Of these techniques, that with the greatest clinical experience is MitraClip implantation in the tricuspid position. Several series have shown that its use in this position is associated with high procedural success rates, few complications, and clear symptomatic improvement.5,6 In the largest series published, the success rate was 97%, with 1 clip in 42% of patients. There were also reductions in the diameter of the tricuspid valve and in pulmonary pressures.6 Failed annuloplasty may be a suitable niche for the use of this device. The MitraClip increases the area of coaptation and, because the length of the leaflets is usually adequate, the use of even 1 clip can provide satisfactory results, as observed in our case. In conclusion, MitraClip implantation in the tricuspid position in patients with recurrent TR after De Vega annuloplasty is a safe and effective technique to reduce TR.
CONFLICTS OF INTERESTR. Estevez-Loureiro is a proctor for MitraClip.
.