Tako-tsubo cardiomyopathy (TTC) is a reversible clinical condition mimicking an acute myocardial infarction. Estrogens may play a protective role: the incidence and prevalence of this entity are higher in postmenopausal women than in men, while occurrence is rare in the pediatric population, as in the case reported herein.
A 12-year-old African girl was scheduled for surgical correction of bilateral flat feet and valgus knee. In childhood, the patient experienced allergic asthma treated with salbutamol. She had no history of cardiac disease and the results of a baseline electrocardiogram was normal (figure 1A). Immediately after intubation, she developed severe desaturation associated with bronchospasm and tachycardia without hemodynamic instability. Intravenous hydrocortisone and nebulized salbutamol were administered. The bronchospasm resolved quickly and the surgical intervention was carried out without further complications.

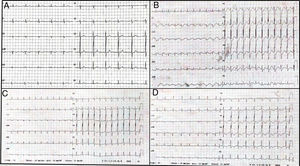
A: the electrocardiogram recorded before the surgical intervention was normal. B: sinus tachycardia and diffuse ST-segment depression during cardiogenic shock. C and D: changes in electrocardiograms showed progressive resolution of the ST-segment and the appearance of widespread, negative T waves.
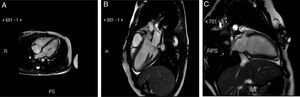
A few minutes after tracheal extubation, the patient developed pulmonary edema and cardiogenic shock. She was then reintubated and transferred to the intensive care unit. An electrocardiogram showed sinus tachycardia and diffuse ST-segment depression (figure 1B). A transthoracic echocardiogram showed marked dilatation of the left ventricle (LV) with akinesia of the mid and apical segments, hyperkinesia of the basal portions of the LV, and severe reduction of left ventricular ejection fraction. Troponin T and pro-brain natriuretic peptide were elevated (275 ng/L and 323 pg/mL, respectively). Subsequently, progressive improvement of the LV function and resolution of the pulmonary edema allowed extubation on the first postoperative day. Daily electrocardiograms showed ST-segment normalization and the appearance of widespread, negative T waves (figure 1C-D), which persisted until discharge. Echocardiography revealed rapid improvement in left ventricular ejection fraction within 2 days after surgery and full recovery at day 15. Magnetic resonance imaging (MRI) was performed 12 days after admission and showed hypokinesia of the apical portions of the LV with minimal, paradoxical telesystolic bulging, no delayed enhancement, and normal left ventricular ejection fraction (figure 2A, B, C). On day 20, the patient was discharged with her antiasthmatic medical therapy only.

In the present case, although we did not perform coronary angiography, the following findings strongly supported the diagnosis of TTC according to the Mayo Clinic criteria:1a) the rapidly reversible peculiar echocardiographic pattern, b) the appearance of repolarization abnormalities on the electrocardiogram, c) the relatively modest troponin elevation, d) the presence of stress triggers (bronchospasm and/or orthopedic surgery), and e) the absence of clinical, laboratory, and instrumental signs of pheochromocytoma or myocarditis. Nevertheless, considering the patient's medical history, her young age and the clinical manifestations, coronary involvement was deemed extremely unlikely. In our case, the patient showed 2 different physical/emotional stressors as potential triggers for the development of TTC: orthopedic surgery and bronchial asthma. In particular, the presence of bronchial hyperactivity might have been crucial. Manfredini et al.2 reported that patients with severe respiratory diseases are at higher risk for the development of TTC and hypothesize a possible relationship with the use of high-dose β2-agonists. The greater myocardial β2:β1 adreno-receptor ratio in the LV apical segments might explain greater responsiveness and vulnerability to the sympathetic stimulation and the higher risk of wall motion abnormalities of these segments. In our case, the patient, who had a marked history of asthma, developed TTC after a sudden episode of intubation-related bronchospasm requiring high doses of β2-agonists: a specific temporal sequence (emotional stress due to the surgical intervention, asthmatic crisis, β2-agonists drugs) leading to the development of the TTC is very likely.
According to the literature,3 the incidence of TTC in children and young adults is fairly rare, but it could be underestimated and misinterpreted as myocarditis or dilated cardiomyopathy, or occasionally classified as “acute ventricular dysfunction of unknown etiology”. From a general point of view, most of the clinical features in terms of triggers, presentation, electrocardiography, and imaging are similar to those in adults. However, several characteristics might be more specific to younger ages. First, in children and young adults, the incidence of coronary artery disease is very rare and therefore coronary angiography is not a first-choice examination, although “nonatherosclerotic” coronary diseases should be considered. Second, in most of the reported cases and/or clinical series in childhood,3 the most frequent clinical presentations are heart failure or cardiogenic shock, rather than chest pain. Finally, in the vast majority of cases, there is full spontaneous recovery of cardiac function, prognosis is better, and, unlike the situation in adults, there are no sex-related differences. Indeed, in older ages, the pattern of complications differs greatly between men and women and the overall prognosis seems to be more severe in men, with worse hemodynamic deterioration and a higher rate of in-hospital mortality.4,5
In the last few decades, cardiac MRI has become more important in the diagnosis of TTC and plays an important role in the younger population. A large, prospective, multicenter study demonstrated that cardiac MRI performed at the initial clinical presentation provided significant functional and anatomical information for the diagnosis of TTC.6 Indeed, our patient, considering her young age and the low risk of coronary artery disease, did not undergo coronary angiography and underwent cardiac MRI, which showed no gadolinium late-enhancement, as is usually observed in TTC.
In conclusion, our case highlights the possible relationship between asthma and TTC. To the best of our knowledge, this is the first reported case of TTC in a young girl following an acute asthma attack during orthopedic surgery and is one of the few reported pediatric patients with TTC who underwent cardiac MRI.