Congenital mitral valve disease is an uncommon condition. Medical treatment can be very complicated in some cases, leaving surgery as the only option. Surgical valvuloplasty often fails in children, especially in neonates and young infants, due to the presence of dysplastic valves with a small annulus and special anatomic features. In such cases, valve replacement is generally the only solution. We present 3 cases of Melody valve implantation in the mitral position.
Patient 1 was a 4-month-old infant weighing 4.6kg with severe mitral regurgitation (MR) (valve with thickened leaflets, reduced mobility, and absence of central coaptation; annulus of 15 mm) that was refractory to medical treatment. Following Kay-Wooler annuloplasty, the boy showed moderate residual MR and was extubated, but he developed severe MR 14 days later and required ventilatory support. We decided to implant a Melody valve in the mitral position using the Boston technique1 with some modifications.2 Before initiation of extracorporeal circulation, the valve was expanded to 18 mm and a 3-mm pericardial sewing cuff was added to the center of the stent using loose sutures anchored to the strut chordae; the triangular struts at the proximal and distal ends of the stent were bent outwards, but the 3 struts supporting the valve commissures were left intact. The mitral valve was exposed using a superior transseptal approach. The posterior leaflet and its subvalvular apparatus and part of the anterior leaflet were resected, sparing the anterosuperior zone with its attachments to the anterior papillary muscle. The mitral prosthesis was crimped (6mm) and attached to the posterior wall of the left ventricle to prevent left ventricular outflow tract (LVOT) obstruction during systole. The pericardial cuff was sutured to the native annulus and the valve was inflated to 4atm with an 18-mm balloon (annulus diameter + 1). The cuff was tied down and the interatrial septum was reconstructed with a fenestrated pericardial patch (Figure 1). An intraoperative transesophageal echocardiogram (TEE) showed grade III periprosthetic MR. The valve was reinflated with a 22-mm balloon, and the outcome was favorable (grade I-II MR). No postoperative complications were observed and the patient was asymptomatic 9 months later. The echocardiogram revealed a mean mitral valve gradient of 3.6 mmHg and grade II periprosthetic MR. No LVOT obstruction was noted.
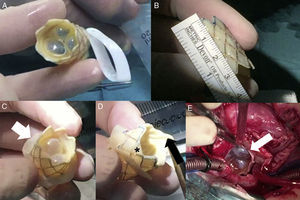
. C: sutured pericardial bovine cuff (arrow). D: triangular struts bent outwards (asterisk); the 3 struts supporting the valve commissures at the distal end are left intact (arrow). E: prosthesis implanted in the mitral position.")
A and B: stented bovine jugular vein graft (Melody valve). C: sutured pericardial bovine cuff (arrow). D: triangular struts bent outwards (asterisk); the 3 struts supporting the valve commissures at the distal end are left intact (arrow). E: prosthesis implanted in the mitral position.
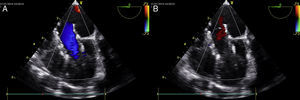
Patient 2 was a 7-month-old girl weighing 4.7kg, who had been treated for complete atrioventricular canal defect at another hospital using the double-patch technique with cleft closure and the Alfieri technique, following pulmonary artery banding. Postoperative clinical course was indolent and the patient required prolonged hospital stay. The infant had a severe double mitral valve lesion and an annulus of 15 mm. She failed to thrive and developed heart failure despite maximum medical treatment. It was decided to implant the Melody valve in the mitral position using the technique described above, with expansion of the prosthesis to 17 mm. Intraoperative TEE showed no evidence of residual MR or LVOT obstruction (Figure 2). The patient was asymptomatic at the 7-month follow-up visit and had no residual lesions (mean gradient, 3mm Hg; no MR).
 and regurgitation (B) with the implanted valve.")
Patient 3 was a 3-kg neonate with congenital aortic valve stenosis (peak gradient, 100 mm Hg). Valvuloplasty had been performed when the child was 2 days old, but the next day, extracorporeal membrane oxygenation was required due to ventricular dysfunction. The neonate was weaned off the oxygenation system after 5 days. The echocardiogram showed a residual aortic stenosis of 50 mmHg, a patent foramen ovale of 4 to 6 mm with a significant left-to-right shunt and moderate MR with structural damage to the leaflets, and an annulus of 15 mm. Progress was not favorable and it was decided to perform a percutaneous aortic valvuloplasty and attempt to close the atrial septal defect. This was not possible, however, because the borders were too loose. After repeated failed attempts at extubation and episodes of low cardiac output, we decided to surgically close the atrial septal defect to force antegrade flow. Extubation, however, was still not possible. As MR appeared to have an important role in the patient's progress, it was decided to replace the mitral valve with a Melody valve expanded to 18 mm. Severe LVOT obstruction due to the prosthesis was observed at the pump outlet and the Ross-Konno procedure was performed immediately. The outcome was favorable, with disappearance of the LVOT obstruction and a normally functioning prosthesis. Postoperative recovery was slow due to lung damage. Two months after surgery the patient had grade II MR.
The search for alternatives to mechanical valve prostheses continues in pediatric settings. Major obstacles to the use of mechanical valves in young patients are a lack of suitably sized valves (the smallest valve available is 16 mm), the need for anticoagulation therapy, and failure to accommodate somatic growth. Different techniques such as supra-annular implantation3 and the chimney mitral valve replacement technique4 have been designed to reduce the risk of thrombosis by preventing the hemidiscs from becoming blocked by surrounding tissue. They do not, however, resolve the other problems mentioned. The Boston group recently described the use of the stented bovine jugular vein graft (Melody valve) in the mitral position.5,6 This device offers several advantages: it can be implanted in very small annuli as it adapts to different diameters; it is theoretically possible to expand the valve percutaneously over time, and it avoids the need for anticoagulants because antiplatelet therapy is sufficient. Our initial experience with the Melody valve has been very positive, although we recognize the need to analyze the short- and mid-term durability of this prosthetic valve.