
Keywords
Received September 24, 2004.Accepted for publication April 21, 2005.
INTRODUCTION
The presence of structural abnormalities in the right atrium (RA) in the newborn establishes a differential diagnosis limited to congenital heart diseases, neoplasms, and thrombi. Remnants of the embryonic venous sinus (VS) are also relevant, because of the high incidence of morphological variants of this structure.
CASE STUDY
We describe the case of a 2-month-old infant with cyanosis at birth.
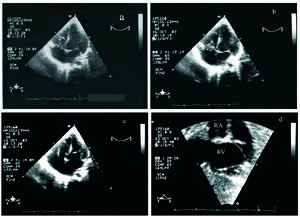
The physical examination disclosed a weight of 3410 g, height 51 cm, blood pressure 100 mm Hg, baseline Sat O2 77%, central cyanosis, tricuspid systolic murmur, mild hepatomegaly, sinus rhythm on electrocardiography, and an enlarged right atrium. The chest x-ray showed a thymic image and low pulmonary flow. Transthoracic echocardiography (TTE) (Figure 1), disclosed a smooth, mobile, redundant tricuspid valve with tense motion that generated a diastolic gradient (5 mm Hg), classified as a dysplastic tricuspid valve. In addition, there was an oval fossa defect (4×6 mm) with right-to-left shunting.

Figure 1. Apical echocardiographic views (diastole [c] systole [a,b]) and inverted subcostal [d]) showing an apparently dysplastic tricuspid valve.
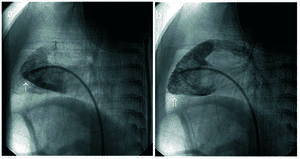
The 50% O2 oximetry values were: systemic 85%, inferior vena cava 69.6%, superior vena cava 70.9%, right atrium 69.5%, pulmonary artery 70.6%, left anterior descending 77%, left ventricle 85.2%. Assuming 95% pulmonary flows, the QP/QS was 0.63. The pressures (mm Hg) were left ventricle 63/-6, right ventricle 22/-7, left atrium 6, right atrium 7, pulmonary artery 23/9/15, aorta 55/29/40. Contrast enhancement of the right ventricle on angiography (Figure 2) showed a double image: one small image adjacent to the tricuspid valve with smooth walls that initially went unnoticed, and another, more distant and larger that presented the classic trabeculation of the right ventricle, with tricuspid competence.

Figure 2. Right ventriculography in left oblique view. Fortuitous injection of contrast material (a) in small cavity (↑), which could be mistaken for a hypoplastic false right ventricle, corresponded to the vestigial cavity. When injected through the tricuspid valve (b), the morphologically normal true right ventricle is defined (↑↑).
Surprisingly, an accessory "pocket-like" tissue with an inlet hole, joined on one side to the tricuspid ring was observed during surgery (Figure 3). The histological study was consistent with fibromyxoid tissue.

Figure 3. Intraoperative image (A) disclosing a "pocket" of supratricuspid accessory tissue (diameter 1.5 cm); a normal tricuspid valve is observed after resection (B).
DISCUSSION
The clinical presentation suggested a diagnosis of cyanotic heart disease, initially characterized as tricuspid dysplasia. Based on the surgical findings, the apparent diagnosis was vestigial remnant of the right valve of the embryonic venous sinus,1 an entity frequently found in conventional imaging tests (30% of the unselected population).2 The mildest form usually consists of a simple structure (eustachian or thebesian valve, terminal crest) or lacelike structure (Chiari's net). In contrast, if the size is large enough to compartmentalize the right atrium, the most serious form is cor triatriatum dexter, an entity classified according to its distribution in the right atrium.1 The clinical symptoms are defined by obstruction (if any) and the associated congenital abnormalities, with hypoplasia of the right ventricle the most frequent.2,3 Between these 2 anatomical variants there is a broad spectrum, depending on the moment at which the venous sinus development was altered.4,5
Infections in this area,6 atrial arrhythmias, paradoxical strokes, and stunted growth due to enteropathy have been described as complications.
In our patient we also ruled out a coronary sinus of atypical distribution (TTE/recirculation).
Papillary fibroelastoma is one of the tumors with similar symptoms. However, unlike the condition in adults, in the pediatric age group it tends to affect the tricuspid valve. The tumor is usually suspected when the typical echocardiographic image is observed.
CONCLUSION
We have presented an unusual form of cyanotic heart disease in an infant, an entity that should be included in the screening for any right atrium structural abnormality.
Correspondence: Dr. J.C. García López.
Orense, 23, 2.o izqda. 02005 Albacete. España.
E-mail: jcgarlo@hotmail.com