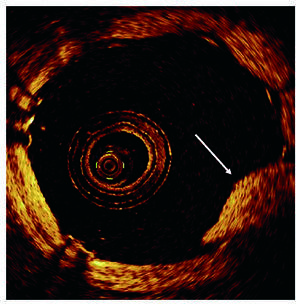
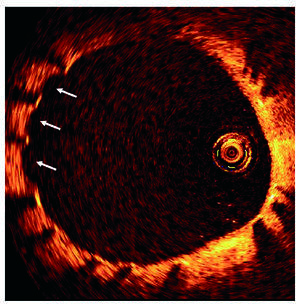
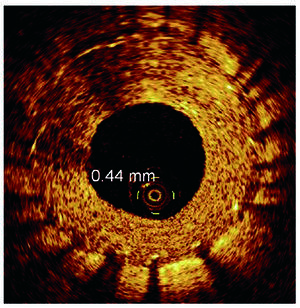
Optical coherence tomography (OCT) is a new intracoronary imaging modality providing images with a resolution 10 times higher than that provided by intravascular ultrasound (IVUS). As the near infra-red light waves used in OCT cannot penetrate blood, we create a blood-free field necessary for imaging by transient occlusion of the vessel proximal to the lesion with a special low pressure balloon catheter followed by saline flushing. The superior imaging capability may be helpful in assessing the efficacy and behaviour of various drug-eluting stents during follow-up. We present a series of OCT images demonstrating features that would be difficult to discern on IVUS. Figure 1 shows the primary implantation of a Cypher sirolimus-eluting stent for in-stent restenosis in the left anterior descending artery (LAD); post-stenting, a tongue of neointimal tissue protruding between the stent struts (single arrow) is clearly seen. Figure 2 shows a 10-month follow-up case of Cypher stenting for a de novo LAD lesion, where a thin layer of neointimal tissue covering the stent struts can be seen. A slight "blown-out" appearance is also demonstrated here (multiple arrows indicating where the vessel wall is slightly concave); we believe this may be an artifact, often seen where the neointimal layer is thin, due to intraluminal pressurization from flushing of a balloon-occluded vessel. Figure 3 shows a case of circumflex artery in-stent restenosis 6 months after implantation of a Taxus paclitaxel-eluting stent; the concentric layer of thick neointimal hyperplasia is well visualized and can be accurately measured.

Figure 1.

Figure 2.

Figure 3.