
Reoperation for mitral bioprosthesis dysfunction is a challenging procedure due to patients’ clinical status and the technical difficulties associated with resecting the prosthesis and implanting a new valve in the weakened mitral annulus; in addition, the redo surgery carries the risk of structural damage to the myocardium and perivalvular leakage.
Transcatheter valve-in-valve implantation into a deteriorated mitral bioprosthesis is a little used technique,1–4 but in complex patients it provides an alternative to conventional surgery that avoids cardiac dissection, extracorporeal circulation, and myocardial ischemia. Most prostheses are implanted via the transapical route because this approach provides direct coaxial access to the valve with shorter delivery catheters; however, another access option is the femoral vein, followed by perforation of the interatrial septum and anterograde valve implantation.
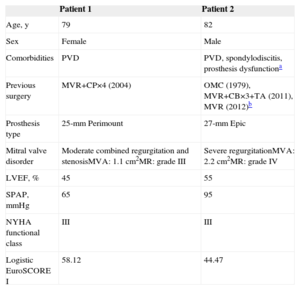
From January 2007 to September 2014, the surgical team at our center performed 70 implantations via the transapical route. In 6 patients, a new valve was implanted in a deteriorated prosthesis: 4 in the aortic position and 2 in the mitral position. The clinical characteristics of the 2 patients selected for the mitral procedure are summarized in the Table.
Baseline Clinical Profile of the 2 Patients
| Patient 1 | Patient 2 | |
|---|---|---|
| Age, y | 79 | 82 |
| Sex | Female | Male |
| Comorbidities | PVD | PVD, spondylodiscitis, prosthesis dysfunctiona |
| Previous surgery | MVR+CP×4 (2004) | OMC (1979), MVR+CB×3+TA (2011), MVR (2012)b |
| Prosthesis type | 25-mm Perimount | 27-mm Epic |
| Mitral valve disorder | Moderate combined regurgitation and stenosisMVA: 1.1cm2MR: grade III | Severe regurgitationMVA: 2.2cm2MR: grade IV |
| LVEF, % | 45 | 55 |
| SPAP, mmHg | 65 | 95 |
| NYHA functional class | III | III |
| Logistic EuroSCORE I | 58.12 | 44.47 |
CB, coronary bypass; LVEF, left ventricular ejection fraction; MR, mitral regurgitation; MVA, mitral valve area; MVR, mitral valve replacement; NYHA: New York Heart Association; OMC, open mitral commissurotomy; PVD, peripheral vascular disease; SPAP, systolic pulmonary arterial pressure; TA, tricuspid annuloplasty.
Both mitral valve implantations were carried out under general anesthesia in the cardiac catheterization laboratory by 2 surgeons and a cardiac catheterization specialist. A left anterior minithoracotomy was performed through the fifth or sixth intercostal space, and transapical access through the pericardial opening was secured by 2 U sutures with teflon-supported 3/0 monofilament suture thread. The ventricular apex was punctured with a guidewire, which was advanced through the opening of the mitral prosthesis into the left atrium. To prevent traumatic perforation of the atrial wall, this guidewire was then exchanged for a preformed high-support guidewire. Coaxial alignment with the ring of the deteriorated bioprosthesis was guided by radiology and echocardiography. This procedure was more challenging with the Epic bioprosthesis because its annulus is only faintly radiopaque; in contrast, the Perimount bioprosthesis, in addition to having a larger annulus, also has a radiopaque supporting stent. After balloon predilatation, an Edwards SAPIEN XT Transcatheter Heart Valve (Edwards Lifesciences, Irvine, California, United States) was implanted in the opposite orientation to that of a transapical aortic valve implant, following the standard protocol with rapid endocardial pacing (Figure). The valve sizes used were 23mm for patient 1 and 26mm for patient 2. These sizes were chosen according to the manufacturer-specified internal diameters of the original bioprostheses, which were consistent with direct measurements by transesophageal echocardiography (23mm for the 25-mm Perimount valve and 24.5mm for the 27-mm Epic valve). In both patients the procedure was completed without technical incident, and correct implantation was confirmed by intraoperative transesophageal echocardiography.
; the arrows mark the position of the coaxially aligned radiopaque bioprosthesis annulus. B: Pre-expanded SAPIEN XT prosthesis; the device can be observed aligned within the radiopaque annulus and supporting stent of the Perimount mitral prosthesis (Edwards Lifesciences, Irvine, California, United States).")
A: SAPIEN XT prosthesis expanded within the degenerated Epic mitral prosthesis (St. Jude Medical, St. Paul, Minnesota, United States); the arrows mark the position of the coaxially aligned radiopaque bioprosthesis annulus. B: Pre-expanded SAPIEN XT prosthesis; the device can be observed aligned within the radiopaque annulus and supporting stent of the Perimount mitral prosthesis (Edwards Lifesciences, Irvine, California, United States).
Patient 1 developed cardiogenic shock in the first hours after implantation, with biventricular dysfunction, acute renal failure, and elevated hepatic enzymes; the condition was reversed by amine therapy and the placement of an intra-aortic counterpulsation balloon for 72hours. The discharge echocardiogram showed normal function of the mitral bioprosthesis, a left ventricular ejection fraction of 35%, and a systolic pulmonary arterial pressure of 70mmHg.
Patient 2 was extubated 8hours after device implantation, and did not require amine therapy at any time. During hospitalization, the patient was treated with intravenous antibiotics for a respiratory infection. The discharge echocardiogram showed normal mitral bioprosthesis function with grade I periprosthetic regurgitation from the posterior commissure, grade II tricuspid regurgitation, and a systolic pulmonary arterial pressure of 65mmHg.
Both patients showed an improvement in New York Heart Association functional class at 12-month follow-up, from class III to class II, and improved hemodynamic parameters at 6-month follow-up:
- •
Patient 1: mitral valve area > 2cm2; maximum velocity, 2. 1 m/s; left ventricular ejection fraction, 30%; systolic pulmonary arterial pressure, 65mmHg.
- •
Patient 2: mitral valve area, 2.2cm2; mean gradient, 8mmHg; left ventricular ejection fraction, 50%; systolic pulmonary arterial pressure, 55mmHg; severe tricuspid regurgitation; no mitral regurgitation.
The first treatment option for a failed biological prosthesis is reoperation, but mitral valve explant surgery carries a number of risks. Transcatheter valve implantation is changing the treatment options for aortic valve disease in patients at high surgical risk, but the potential role of the transcatheter approach remains unclear in the treatment of failed bioprosthetic valves in the mitral position.
In our study, we selected 2 high-risk patients excluded from conventional surgery. Although the early postoperative outcomes differed, the clinical progress of both patients was positive, even in the presence of multiple comorbidities. Left ventricular dysfunction continues to be a risk in mitral valve repair because ventricular function is often overestimated in patients with mitral regurgitation,5 which might partly explain the initially poor postoperative outcome in patient 1. In our opinion, management options for such patients should include the presurgical deployment of an intra-aortic counterpulsation balloon and therapy with inotropic drugs in the first hours after valve implantation. These measures, once introduced, dramatically improved clinical progress in patient 1.
In conclusion, transcatheter valve-in-valve implantation in a deteriorated mitral biosprosthesis via the transapical route is a feasible procedure that is becoming established as an alternative therapeutic option for patients at high or prohibitive surgical risk.