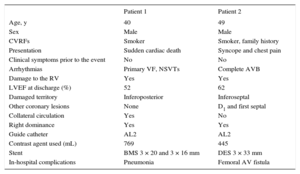
An anomalous origin of the right coronary artery (RCA) in the left sinus of Valsalva is an anatomic variant associated with ischemia, infarction, and sudden cardiac death in young patients.1 The prevalence of this anomaly ranges from 0.026% to 0.92% in analyzed series, typically invasive and noninvasive coronary angiography registries. This type of coronary anomaly is related to an increased presence of anatomical characteristics associated with worse prognosis, such as an interarterial or intramural course, smaller ostial diameter, and acute takeoff angle.2 However, there have been few cases of acute coronary syndrome related to an anomalous RCA. We present 2 such patients treated in our center (Table).
Patient Characteristics
| Patient 1 | Patient 2 | |
|---|---|---|
| Age, y | 40 | 49 |
| Sex | Male | Male |
| CVRFs | Smoker | Smoker, family history |
| Presentation | Sudden cardiac death | Syncope and chest pain |
| Clinical symptoms prior to the event | No | No |
| Arrhythmias | Primary VF, NSVTs | Complete AVB |
| Damage to the RV | Yes | Yes |
| LVEF at discharge (%) | 52 | 62 |
| Damaged territory | Inferoposterior | Inferoseptal |
| Other coronary lesions | None | D1 and first septal |
| Collateral circulation | Yes | No |
| Right dominance | Yes | Yes |
| Guide catheter | AL2 | AL2 |
| Contrast agent used (mL) | 769 | 445 |
| Stent | BMS 3 × 20 and 3 × 16 mm | DES 3 × 33 mm |
| In-hospital complications | Pneumonia | Femoral AV fistula |
AV, arteriovenous; AVB, atrioventricular block; BMS, bare-metal stent; CVRFs, cardiovascular risk factors; D1, first diagonal; DES, drug-eluting stent; LVEF, left ventricular ejection fraction; NSVTs, nonsustained monomorphic ventricular tachycardias; RV, right ventricle; VF, ventricular fibrillation.
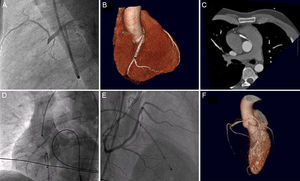
The first patient was a 40-year-old man who had been resuscitated after out-of-hospital sudden cardiac arrest due to ventricular fibrillation. He received basic and advanced resuscitation for 1 hour and had inferior ST-elevation on electrocardiography. Coronary angiography failed to identify obstructive lesions in the left coronary system. The RCA was not visualized, even after multiple contrast agent injections into the right sinus, ventriculography, and aortography. The origin of the artery was finally located in the left sinus and imaging revealed complete proximal thrombotic obstruction (Figure 1A). Implantation of 2 bare-metal stents achieved a good angiographic result. After therapeutic hypothermia, the patient showed no neurological sequelae. Computed tomography (CT) showed an interarterial course (Figure 1B and Figure 1C). At discharge, the patient was enrolled in a cardiac rehabilitation program and underwent repeat definitive and negative ischemic stress tests. Surgical correction of the coronary anomaly was rejected due to the absence of symptoms prior to the event and subsequent ischemia induction.

A: catheterization of the right coronary artery in the left sinus in a lateral projection. B: three-dimensional reconstruction showing the interarterial course of the anomalous right coronary artery. C: detail of the origin of the right coronary artery in an axial plane. D: nonselective angiography after successful thrombolysis. E: selective catheterization with a severe residual lesion. F: three-dimensional reconstruction showing the vessel origin in the left sinus.
The second patient was a 49-year-old man who was transferred to our center due to chest pain and syncope. An electrocardiogram showed complete atrioventricular block with a narrow QRS escape rhythm and ST-segment elevation in inferior and right leads. Coronary angiography showed no obstructive lesions in the left coronary system. Because the RCA could not be identified with multiple contrast agent injections and aortography, intravenous thrombolysis was performed in the catheterization laboratory. After successful coronary reperfusion, repeat contrast agent injection revealed a RCA with a high origin outside of the right sinus (Figure 1D). The patient had a severe residual lesion at the proximal-medial area (Figure 1E) that was treated with a drug-eluting stent. Computed tomography confirmed the origin of the RCA in the left sinus, as well as an interarterial course (Figure 1F). Stress echocardiography was performed. Although inconclusive, it was negative, even at very high intensities, and surgery was ruled out for the same reasons as in the first patient.
An anomalous origin of the RCA with interarterial course is a known risk factor for sudden cardiac death in young patients. The most accepted theories for this association suggest that the particular anatomic structure of the artery can provoke an ischemic event that triggers ventricular arrhythmias.3 The incidence of atherosclerosis in coronary artery anomalies is similar to or lower than that of anatomically normal arteries, and intravascular ultrasound studies have failed to identify atherosclerotic disease in the initial intramural segment of these vessels, which is generally the site of greatest stenosis.4,5 Nonetheless, both cases demonstrate that plaque rupture or erosion with thrombus formation is one of the possible mechanisms of sudden cardiac death and cardiac events in this patient population.
An inability to visualize the RCA during coronary angiography should suggest the presence of this coronary anomaly. Systemic thrombolysis should be considered in these patients to locate the origin, as well as facilitated angioplasty (as in the second patient). If there are contraindications (such as recent traumatic resuscitation), catheterization of the contralateral sinus should be attempted, as well as atypical projections and aortography if necessary. Series detailing interventions for anomalous RCAs show that single stents can be implanted in these vessels, with promising clinical and angiographic results.5 Nonetheless, these procedures involve prolonged and technically complex catheterizations requiring a high volume of contrast agent.
Clinical practice guidelines indicate surgical revascularization for patients with an anomalous RCA and interarterial course if there are symptoms or documented ischemia, but the treatment is controversial in other patients6 and there is no widely accepted approach. Both in our patients and in the few previously described cases, the culprit lesions were outside the interarterial course. This situation adds another point of uncertainty regarding its further evaluation, suggesting the possible need for various surgical techniques to free the vessel course.
CONFLICTS OF INTERESTÁ. Sánchez-Recalde is an Associate Editor of Revista Española de Cardiología.