The surgical palliation first described by Fontan and Baudet1 as Fontan-type operation or total cavopulmonary connection (TCPC) is based on a connection between the systemic venous system and the pulmonary artery tree, excluding the pumping function of the main ventricle. Under these circumstances, the main ventricular chamber acts as a single ventricle, supplying anterograde flow and aspirating systemic venous and pulmonary vein return. The pressure difference between the systemic venous reservoir and the main ventricle is key to promoting flow in that direction. As a result, the low pressures of the pulmonary vascular circuit are determinants of cardiac output. Patients with a mean pulmonary artery pressure>15 mmHg and pulmonary resistance>2 U/m2 are considered to be at risk for this condition.2,3 Any drug that lowers pulmonary resistances will increase pulmonary flow, ventricular filling, and systolic volume.4 Sildenafil is a phosphodiesterase-5 inhibitor that increases intracellular cyclic guanosine monophosphate and exerts a selective vasodilator effect on the pulmonary vasculature; it is used in patients with pulmonary hypertension. Its pharmacokinetic and hemodynamic effects are effective in patients with a single-ventricle pathophysiology who present signs of Fontan dysfunction.5,6 The literature contains no description of the preoperative use of sildenafil to reduce pulmonary hypertension to feasible values for the Fontan procedure. Nevertheless, many groups use the drug empirically for Fontan candidates when the hemodynamic evidence of pulmonary hypertension indicates that the operation should not be performed.
We describe our experience with the use of sildenafil in 3 pediatric patients at high hemodynamic risk for single-ventricle circulation prior to TCPC.
In these children, the underlying congenital heart disease was tricuspid atresia Ib (9 months, Blalock-Taussig shunt), double-outlet of the left ventricle and interrupted aortic arch (5 days, aortic repair and pulmonary banding), and double-outlet of the left ventricle and aortic coarctation (coarctectomy and pulmonary banding). All patients underwent bidirectional Glenn shunt at 5 years, 5 months, and 4 years, respectively.
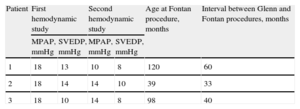
The subsequent clinical course, based on the hemodynamic study, showed that they would not be good TCPC candidates (Table).
Hemodynamic Variables and Age
| Patient | First hemodynamic study | Second hemodynamic study | Age at Fontan procedure, months | Interval between Glenn and Fontan procedures, months | ||
| MPAP, mmHg | SVEDP, mmHg | MPAP, mmHg | SVEDP, mmHg | |||
| 1 | 18 | 13 | 10 | 8 | 120 | 60 |
| 2 | 18 | 14 | 14 | 10 | 39 | 33 |
| 3 | 18 | 10 | 14 | 8 | 98 | 40 |
MPAP, mean pulmonary artery pressure; SVEDP, single ventricle end-diastolic pressure.
Sildenafil (50-mg tablets) was administered at oral doses of 4-6 mg/kg/day for 6 months after catheterization that showed high pulmonary pressures for TCPC. After receiving pulmonary vasodilator therapy, the patients showed lower pulmonary and end-diastolic pressures of the main ventricle, and TCPC was indicated and performed. Both hemodynamic studies were carried out under general orotracheal anesthesia at FiO2 0.21, and the patient was disconnected from the mechanical ventilator when the pressures were recorded.
In patients 1 and 2, the on-pump arrested-heart modified Fontan operation was performed using a fenestrated intra-atrial tunnel; patient 3 received a bilateral nonfenestrated cavopulmonary extracardiac connection with a polytetrafluorethylene tube with an 18-mm diameter.
None of the patients showed TCPC dysfunction during the postoperative period. Patient 3 experienced a neurologic lesion without TCPC dysfunction and died. The other 2 patients show good Fontan outcome after more than 1 year of follow-up with no complications. Sildenafil was discontinued 3 months after hospital discharge, and no drug-induced adverse effects were observed.
The hemodynamic status of all 3 patients improved when they were treated with the pulmonary vasodilator, and TCPC was well tolerated up to 1 year after the procedure; however, in all 3 children the single ventricle was of left morphology and, therefore, a subgroup of single ventricles that has proven to have a better clinical prognosis and possibly better tolerance and therapeutic response.
Sildenafil therapy could be a useful therapeutic tool for patients at high hemodynamic risk for the Fontan procedure. We believe that randomized studies with a sufficient number of patients and homogeneity of groups in variables of possible influence are needed to establish the usefulness of sildenafil in these cases.
.