
Giant right atrium (RA) aneurisms and diverticula are uncommon congenital anomalies,1 although their true incidence is difficult to estimate since small malformations may go unnoticed.2
A 70-year-old man, with permanent atrial fibrillation and a diagnosis of “possible cor triatriatum dexter” 15 years previously, was admitted to hospital for suspected coronary disease; coronary angiography showed no significant lesions in the coronary arteries. A transthoracic echocardiogram was performed, which placed the previous diagnosis in doubt due to the finding of an echolucent cavity adjacent to the RA and right ventricle (Fig. 1A). The cavity was confirmed by transesophageal echocardiography, compatible with a diagnosis of giant RA diverticulum. The size of the diverticulum was approximately twice that of the RA and extended from the inferior border of the inferior vena cava to 20-mm distal to the tricuspid annulus (Fig. 2A). No hemodynamic effects due to the presence of the diverticulum, collapse of the right cavities or dilation of the vena cavae were observed. Tricuspid flow was normal. Injection of an ultrasonographic contrast agent (sulphur hexafluoride) revealed a communication between the cavity and cardiac structures (Fig. 1B) through a defect in the free wall of the RA (Figs. 1C and D and Fig. 2B). Given the scarce clinical repercussion of the anomaly, conservative management was provided, with no relevant incidents in a 2-year follow-up.
 on 3-dimensional real-time transthoracic echocardiography, subcostal bicaval plane. D: Passage of ultrasound contrast material (arrow) between the right atrium and diverticulum after injection into the left antecubital vein. D, diverticulum; LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle; VC, superior vena cava.")
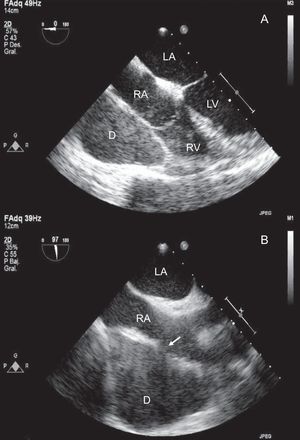
Transthoracic echocardiography. A: Echolucent cavity adjacent to the right atrium and ventricle in the apical 4-chamber plane. B: Filling of the chamber after injection of the ultrasound contrast agents, showing the relationship of the chamber with the cardiac cavities. C: Communication between the right atrium and diverticulum (arrow) on 3-dimensional real-time transthoracic echocardiography, subcostal bicaval plane. D: Passage of ultrasound contrast material (arrow) between the right atrium and diverticulum after injection into the left antecubital vein. D, diverticulum; LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle; VC, superior vena cava.
. D, diverticulum; LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle.")
Diverticula are the third most frequent malformations of the RA, after congenital atrial enlargement and coronary sinus aneurysm,2 and a possible genetic cause has been proposed, based on a report of an affected family.3 The diverticulum does not contain all the layers of the atrial wall, since it communicates with the RA via a defect in its free wall or in the appendage, which are very thin.
These anomalies are frequently asymptomatic but can be associated with atrial tachyarrhythmia,4,5 as in our case. Likewise, several cases associated with Wolff-Parkinson-White syndrome have been described,6 in which contact between the diverticular wall and the right ventricle may allow ample electrical communication between the atrial and ventricular myocardium, without there being a well-defined accessory pathway. Giant diverticula may produce thoracic pain and compressive symptoms, such as peripheral edema, enlarged liver or jugular engorgement.4 Progressive RA dilation, thrombus formation and rupture of the diverticulum have also been described, with an estimated incidence of sudden death of 6%.2
Surgical resection is indicated in refractory atrial tachyarrhythmias, thromboembolic phenomena and compressive symptoms. In asymptomatic patients, the optimal approach is controversial; some authors adopt a conservative approach,1 as in our case. Due to the risk of sudden death from rupture of the diverticulum, some authors advocate surgical resection of giant diverticula.3,4
The diagnosis is given by echocardiography and, in addition to aneurysm, the differential diagnosis includes Ebstein's anomaly. The use of contrast-enhanced ultrasound is highly useful since it allows the relationship between the cavity and the RA to be established and provides information on the site and anatomical characteristics of the communication. Due to its accessibility, good tolerability and low cost, this technique can be considered the diagnostic procedure of choice. In selected patients, computed tomography or magnetic resonance can help in the differential diagnosis with pericardial cysts or mediastinal tumors.4
Although injection of agitated saline serum can be used to opacify the right cavities, it is unlikely to completely fill the cavity in giant diverticula, nor is it useful if the diverticulum communicates with the left cavities and consequently the use of a transpulmonary contrast agent seems to be the best option.
The present article constitutes the first description of the utility of contrast-enhanced ultrasound in the diagnosis of a giant RA diverticulum.
.