
Large studies have been carried out in Spain to determine the prevalence of atrial fibrillation (AF) in the general population,1,2 but they do not include individuals younger than 40 years. Hence, the available epidemiologic data in this age group are very limited. The aim of this study was to determine the prevalence of AF in a large sample of the Spanish working population, with particular emphasis on the subgroups younger than 40 years of age.
The present report applies the methods used in the previously published ICARIA (Ibermutuamur CArdiovascular RIsk Assessment) study.3 ICARIA reported the results of a cohort of 13179 workers aged 16 to 74 years from 5 Spanish regions (Madrid, Valladolid, Murcia, Malaga, and Asturias), who underwent a medical check-up between May 2008 and November 2010, including a 12-lead resting electrocardiogram. In the present study, also of an observational, cross-sectional nature, we calculated the percentages of workers with AF in the total sample and in subgroups stratified by sex and age.
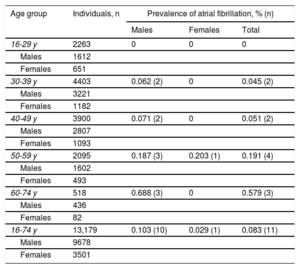
The general characteristics of the sample are shown in Table 1. There was a statistically significant association between AF and age, diabetes, high blood pressure, obesity, high risk according to the Framingham score, and lower high-density lipoprotein cholesterol levels. Percentages of AF in the various subgroups are shown in Table 2. The prevalence of AF in the overall sample was 0.083%, and 10 of every 11 recordings showing this arrhythmia were in men. In the 30- to 39-year-old age group, 2 recordings showed AF in 2 men, aged 38 and 39 years, respectively, which yielded a prevalence of 0.045% in this age group. Among 2263 workers aged 16 to 29 years, no AF cases were observed.
Demographic Characteristics, Work Sector, and Risk Factors of Workers With and Without AF
| Characteristics | Total sample (n = 13179) | Workers without AF (n = 13168) | Workers with AF (n = 11) | P |
|---|---|---|---|---|
| Males | 73.4 | 73.4 | 90.9 | .3314 |
| Age, y | 40 ± 10.5 | 40 ± 10.5 | 52.5 ± 11.1 | .0001 |
| Age groups | .0077 | |||
| 16-29 y | 17.2 | 17.2 | 0 | |
| 30-39 y | 33.4 | 33.4 | 18.2 | |
| 40-49 y | 29.6 | 29.6 | 18.2 | |
| 50-59 y | 15.9 | 15.9 | 36.4 | |
| 60-74 y | 3.9 | 3.9 | 27.3 | |
| Manual worker | 53.6 | 53.6 | 63.6 | .7143 |
| Nonmanual worker | 46.4 | 46.4 | 36.4 | |
| Work sector | .6253 | |||
| Agriculture | 0.4 | 0.4 | 0 | |
| Industry | 14.7 | 14.7 | 10 | |
| Construction | 23.5 | 23.5 | 10 | |
| Services | 61.4 | 61.4 | 80 | |
| Smokera | 38.5 | 38.5 | 50 | .6738 |
| Diabetes mellitusb | 2.3 | 2.2 | 30 | <.0001 |
| Hypertensionc | 20 | 19.9 | 54.5 | .0126 |
| Systolic pressure, mmHg | 124.1 ± 15.7 | 124.1 ± 15.7 | 127.5 ± 14 | .4729 |
| Diastolic pressure, mmHg | 77 ± 10.8 | 77 ± 10.8 | 79.2 ± 6.5 | .4942 |
| BMI, kg/m2 | 26.2 ± 4.2 | 26.2 ± 4.2 | 29.7 ± 5.1 | .0060 |
| Obesity, BMI ≥30 | 16.4 | 16.4 | 54.5 | .0026 |
| Morbid obesity, BMI ≥ 40) | 0.5 | 0.5 | 0 | 1 |
| Dyslipidemiad | 55.4 | 55.4 | 90 | .0597 |
| Total cholesterol, mg/dL | 196.2 ± 37.2 | 196.3 ± 37.2 | 182.8 ± 40.1 | .2531 |
| HDLc, mg/dL | 55.3 ± 14.9 | 55.3 ± 14.9 | 43.9 ± 19.3 | .0152 |
| LDLc, mg/dL | 120.5 ± 32.9 | 120.5 ± 32.9 | 115.9 ± 28.1 | .6589 |
| Triglycerides, mg/dL | 110.2 ± 83.7 | 110.2 ± 83.7 | 126.3 ± 50.1 | .5435 |
| Scoree | .0022 | |||
| Low | 93.9 | 93.9 | 55.6 | |
| Moderate | 1.1 | 1.1 | 0 | |
| High | 5 | 5 | 44.4 | |
AF, atrial fibrillation; BMI, body mass index; HDLc, high-density lipoprotein cholesterol; LDLc, low density lipoprotein cholesterol.
Values are expressed as the percentage or the mean ± standard deviation.
Diabetes type I and/or II and/or receiving insulin therapy and/or glycemia ≥ 126mg/dL at the medical check-up.
Previous diagnosis of hypertension and/or receiving antihypertensive therapy and/or systolic pressure >140mmHg and/or diastolic pressure >90mmHg at the medical check-up.
Prevalence of Atrial Fibrillation by Age Groups and Sex
| Age group | Individuals, n | Prevalence of atrial fibrillation, % (n) | ||
|---|---|---|---|---|
| Males | Females | Total | ||
| 16-29 y | 2263 | 0 | 0 | 0 |
| Males | 1612 | |||
| Females | 651 | |||
| 30-39 y | 4403 | 0.062 (2) | 0 | 0.045 (2) |
| Males | 3221 | |||
| Females | 1182 | |||
| 40-49 y | 3900 | 0.071 (2) | 0 | 0.051 (2) |
| Males | 2807 | |||
| Females | 1093 | |||
| 50-59 y | 2095 | 0.187 (3) | 0.203 (1) | 0.191 (4) |
| Males | 1602 | |||
| Females | 493 | |||
| 60-74 y | 518 | 0.688 (3) | 0 | 0.579 (3) |
| Males | 436 | |||
| Females | 82 | |||
| 16-74 y | 13,179 | 0.103 (10) | 0.029 (1) | 0.083 (11) |
| Males | 9678 | |||
| Females | 3501 | |||
Published data are scarce on the prevalence of AF in Spanish adults younger than 40 years, which hampers comparison of our findings with those of other studies. The REGICOR4 study included 1748 randomly selected men and women from the general population of Girona. The main limitation of that study was the small sample size: 273 individuals in the group aged 25 to 34 years and 341 in the group aged 35 to 44 years. An AF prevalence of 0.4% was found in the first age range, and there were no AF cases in the second. The rate observed in the 25- to 34-year-old group, presumably much higher than would be expected in the reference population, was reached because a single AF case was detected in 1 man. The DARIOS5 study jointly analyzed the data from 6 studies performed in random samples of the general population of Barcelona, Canary Islands, Balearic Islands, Extremadura, Girona, and Toledo. The prevalence of AF in 4018 individuals aged 18 to 45 years was 0.05% (1 man and 1 woman). In this case, the main limitation was the absence of data to enable estimation of prevalence in age-related subgroups within the wide range of 18 to 45 years. The study by Carro-Hevia et al.6 in Asturias also points to a low rate of AF in the young Spanish population, as no cases were detected on electrocardiography performed in 1220 federated athletes aged 15 to 29 years.
The interpretation of the results in this study has several limitations. Because of the methods used, it is likely that cases of transient AF were not detected. It should be noted that paroxysmal AF is particularly more common in the young population than persistent or permanent AF. This, together with the working nature of the sample, which excludes individuals with disabling heart disease, precludes extrapolation of the rates observed to the overall Spanish population and may be the reason why our rates are lower than those reported in the OFRECE1 study in comparable age ranges. Furthermore, individuals from only 5 Spanish regions were included; hence, the data obtained do not represent the entire working population of Spain. The paucity or absence of cases in the age groups younger than 40 years indicates that the sample size does not suffice to provide a precise estimate of the prevalence of AF in the entire Spanish working population in these ages.
In conclusion, the present report analyzes the prevalence of AF in a Spanish working population cohort with a large representation of adults younger than 40 years, which contrasts with most previous studies performed in our country. Nonetheless, the small number of cases detected in those aged 40 years and younger indicates that a larger sample would be needed to achieve precise estimation of the AF prevalence in the younger Spanish working population, and this would likely be true for other samples of apparently healthy young individuals.
FUNDINGGrant PI-0095-CS 2005, Ministry of Health, Government of Andalusia.
.