We present the case of a 76-year-old man who was urgently hospitalized for syncope. The electrocardiogram documented atrial fibrillation with high-grade atrioventricular block. The patient's clinical history included hypertensive heart disease with moderate ventricular dysfunction and permanent atrial fibrillation, as well as a chest deformity due to kyphoscoliosis.
During hospitalization, the absence of drugs or analytical abnormalities that could explain the clinical picture was confirmed, and tests showed left ventricular dilatation and dysfunction (ejection fraction = 40%) with normal coronary arteries. Continuous monitoring provided evidence of atrial fibrillation with preserved atrioventricular conduction, but with symptomatic paroxysmal episodes of high-grade block that required isoproterenol administration; a definitive single-chamber pacemaker was indicated. During the implantation procedure, marked venous tortuosity (Figure 1A), related to anterior displacement of the heart due to the barrel chest deformity (Figure 1B), made it impossible to advance the electrode to the superior vena cava from either a right or left approach. The alternative, epicardial implantation, was ruled out because of the patient's frail clinical status and the drawbacks of a procedure requiring general anesthesia. We decided to implant a leadless pacemaker (Micra, Medtronic Ibérica SA; Madrid, Spain) using a right femoral approach. Computed tomography angiographic study of the venous system showed distortion of the abdominal organs, a polycystic liver, and a large diaphragmatic hiatal hernia, whereas the femoral and abdominal venous system was confirmed to be accessible (Figure 1C). The implantation procedure progressed without incident from the access to the right atrium, with some difficulty releasing the device because of the position of the heart (right atrial dilatation, ventricular dilatation, and anterior elongation of the inferior vena cava-right atrial junction). The device was placed in the apical area of the right ventricle with no complications and with good parameters (sensing = 11 mV, impedance = 600 Ω, threshold 0.75 V to 0.24 ms). It was programmed in VVI mode at 50 bpm (Figure 2). The patient was discharged at 24hours following the procedure without incident. The device parameters were confirmed to be stable over follow-up.
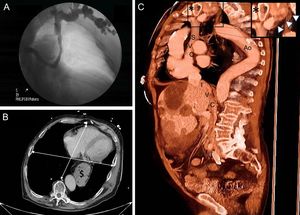
; a diaphragmatic hiatal hernia ($) is visible. C: Thoracoabdominal CT angiography sagittal image showing vascular distortion; in the enlarged image of the area of interest (asterisk), siphon configuration of the left subclavian vein (arrowheads). Ao, aorta; CT, computed tomography; IVC, inferior vena cava; SVC, superior vena cava.")
A: Anteroposterior venography of the left subclavian vein showing a tortuous course up to the superior vena cava. B: Chest CT transverse slice depicts barrel chest deformity causing a large separation of the heart from the descending aorta; the transverse:anteroposterior chest diameter ratio was 1.3 (normal 2.5); a diaphragmatic hiatal hernia ($) is visible. C: Thoracoabdominal CT angiography sagittal image showing vascular distortion; in the enlarged image of the area of interest (asterisk), siphon configuration of the left subclavian vein (arrowheads). Ao, aorta; CT, computed tomography; IVC, inferior vena cava; SVC, superior vena cava.
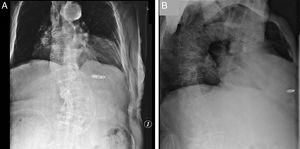
 and lateral (B) chest radiographs showing the final position of the device.")
Conventional transvenous pacemaker implantation is currently the treatment of choice for symptomatic bradycardia. The procedure requires a central venous access, usually a thoracic vein (subclavian, axillary, or cephalic), as this technique provides high success rates and good long-term outcomes.1 However, these access routes are sometimes unavailable because of stenosis or local complications such as infection. In the patient reported, manipulation of the electrode was unfeasible because of tortuosity of the thoracic venous system. Barrel chest is a thoracic cage deformity resulting from horizontalization of the ribs that leads to an increase in the anteroposterior diameter of the thorax relative to the lateral diameter. It is commonly seen in older persons with osteoarthritis of the dorsal column, and has been classically described in patients with advanced pulmonary emphysema. In severe forms, the deformity causes very abnormal positioning of the thoracic organs and their relationships with other systems. In our patient it resulted in a voluminous hiatal hernia and anterior displacement of the heart relative to the large vessels, with adaptation of the arterial and venous systems through marked elongation and tortuosity of the intrathoracic vessels.
Several studies have reported that leadless pacemakers are safe and effective in the general population requiring single-chamber pacing, with high success rates and good mid-term outcomes.2,3 These devices can also be a solution for patients with complications at the usual access routes (infection, lead breakage, or venous stenosis).4 Our case involving a patient with a severe chest deformity provides a clear, new example of the advantages of a leadless device over options requiring standard access routes (epicardial or femoral), which are more invasive and imply greater vulnerability of the pacing system. Use of a steerable sheath over a guide catheter to reach the right atrium allows better stability and maneuverability despite anatomic distortions. We believe that leadless pacemakers could be considered as a first-line option in patients with severe chest deformities requiring single-chamber pacing, as they additionally allow prompt hospital discharge without convalescence following the procedure.
.