Multidetector computed tomography (MDCT) is an established noninvasive technique that enables evaluation of calcium deposit and stenosis of the coronary arteries.1 Some authors have assessed the overall correlation between MDCT and invasive coronary angiography (ICA). MDCT has shown good performance for detecting coronary disease (CD), with a tendency to identify a larger atherosclerotic burden, particularly in the proximal segments.2 However, there are no studies correlating the severity of coronary lesions assessed by these two techniques.
The objective of this study was to determine the diagnostic performance of MDCT in each coronary segment, using quantitative coronary analysis (QCA) of stenosis detected on ICA as the reference pattern.
We analyzed 1648 segments in 103 patients with a previous MDCT examination referred for ICA between November and March 2019. The inclusion criteria were age ≥ 18 years, stable clinical status, and radial artery access, where vasodilators were administered at the start of the procedure. We did not exclude patients with a history of ischemic heart disease, previous stents, atrial fibrillation, and elevated coronary artery calcium (CAC) score (Agatston> 400), for which some studies have shown a good diagnostic yield for MDCT.3 The study was approved by the hospital ethics committee, and informed consent for participation was obtained from all patients (CEIm code: 19.03.1384-GHM).
MDCT was performed on 160-detector and 320-detector Toshiba systems (Toshiba Medical Systems, Japan) (61 and 42 imaging studies, respectively), and images were evaluated by experienced cardiologists (> 1000 MDCT/year). Significant CD was defined as stenosis ≥ 50%: moderate between 50% and 70%, and severe> 70%.
Lesion quantification by ICA involved a deferred, masked analysis performed with the QCA software package provided in the Philips Medical System Integris Allura Xper FD-20. Measurements were done in the projection showing maximum angiographic stenosis, in end-diastole, with calibration of the diagnostic catheter (figure 1). The classification in the modified American Heart Association model was used for coronary segmentation.4
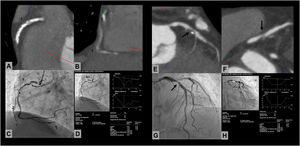
 and invasive coronary angiography (ICA). The series of images at the left shows a right middle coronary artery lesion that is not assessable on MDCT in a patient with a calcium score > 2000. On quantitative coronary analysis (QCA), stenosis was 92%. The series on the right shows an example of a good correlation between MDCT and QCA in a patient with a focal lesion in the proximal left anterior descending artery (arrow).")
Correlation analysis between multidetector computed tomography (MDCT) and invasive coronary angiography (ICA). The series of images at the left shows a right middle coronary artery lesion that is not assessable on MDCT in a patient with a calcium score > 2000. On quantitative coronary analysis (QCA), stenosis was 92%. The series on the right shows an example of a good correlation between MDCT and QCA in a patient with a focal lesion in the proximal left anterior descending artery (arrow).
The mean age of the population was 67 years, 78% were men, and hypertension was the most prevalent risk factor. The mean CAC score was 782±1034 [23-4523], and 14% of patients had a CAC score> 400. The mean heart rate during image acquisition was 66 bpm.
Of the 1648 coronary segments analyzed, 1549 (94%) could be assessed, and MDCT was considered of good quality in 96 patients (93%). Among segments that could not be assessed (n=99), the most frequent were the mid- and distal right coronary artery, and 84% were in patients with a CAC score> 100. MDCT was rated suboptimal in 7 patients: 5 had a CAC score> 1000, and 2 had an elevated heart rate at image acquisition.
In the MDCT images, CD was detected in 53.2% (824/1549) of the segments evaluated; stenosis was mild in 6% (50/824), moderate in 63% (519/824), and severe in 31% (255/824).
As to the ICA evaluation, QCA was performed in 889 lesions: stenosis was mild in 8% (69/889), moderate in 60% (531/889), and severe in 32% (289/889). In total, 98 significant lesions (≥ 50%) were detected on ICA, but not on MDCT; 67 of these (68%) were located in the distal segments (distal left anterior descending artery and distal right coronary-posterior descending artery).
In the analysis by segments, excellent correlations (κ> 0.81) were found for most segments. Correlations were good (κ between 0.61 and 0.80) for the main coronary, mid-right coronary artery, distal left anterior descending, and distal posterior descending, with MDCT showing a tendency to overestimate the degree of stenosis in the main coronary and mid-right coronary arteries, and underestimate lesions in the distal segments (table 1).
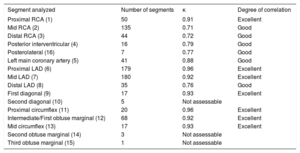
Correlation study: stenosis quantified by multidetector computed tomography vs invasive coronary angiography in each of the coronary segments
| Segment analyzed | Number of segments | κ | Degree of correlation |
|---|---|---|---|
| Proximal RCA (1) | 50 | 0.91 | Excellent |
| Mid RCA (2) | 135 | 0.71 | Good |
| Distal RCA (3) | 44 | 0.72 | Good |
| Posterior interventricular (4) | 16 | 0.79 | Good |
| Posterolateral (16) | 7 | 0.77 | Good |
| Left main coronary artery (5) | 41 | 0.88 | Good |
| Proximal LAD (6) | 179 | 0.96 | Excellent |
| Mid LAD (7) | 180 | 0.92 | Excellent |
| Distal LAD (8) | 35 | 0.76 | Good |
| First diagonal (9) | 17 | 0.93 | Excellent |
| Second diagonal (10) | 5 | Not assessable | |
| Proximal circumflex (11) | 20 | 0.96 | Excellent |
| Intermediate/First obtuse marginal (12) | 68 | 0.92 | Excellent |
| Mid circumflex (13) | 17 | 0.93 | Excellent |
| Second obtuse marginal (14) | 3 | Not assessable | |
| Third obtuse marginal (15) | 1 | Not assessable |
RCA, right coronary artery; LAD, left anterior descending artery.
The overall sensitivity of MDCT for detecting significant CD, using QCA on ICA as the reference pattern, was 90.5%, with a specificity of 89.8%, positive predictive value of 90.1%, and negative predictive value of 90.3%. Eighty-two lesions showing ≥ 50% stenosis on MDCT were not significant in the ICA QCA analysis (false positives) and 78 lesions showing ≥ 50% stenosis on ICA were not significant on MDCT (false negatives). The net diagnostic yield of MDCT (estimated by ROC curve) was 0.95 (95% confidence interval 0.92-0.97).
In this study, MDCT was suitable for quantifying stenosis of the major coronary vessels, using QCA on ICA as the reference, even in patients with previous stents, coronary calcification, or atrial fibrillation, with the greatest limitation in the assessment of distal lesions. To our knowledge, this is the first study to carry out a correlation analysis between these 2 techniques for each coronary segment in an unselected study population.
FUNDINGL. Fernández-Friera received a grant from Carlos III Health Institute, Spain (PI15/02019). L. Fernández-Friera and A. Moreno-Arciniegas received a grant from the Community of Madrid, Spain (AORTASANA-CM; B2017/BMD-3676), European Social Fund (ESF).