
Stress cardiomyopathy, tako-tsubo syndrome, and transient apical dyskinesia1 are names given to a cardiac syndrome commonly characterized by left ventricular systolic dysfunction generally involving the apical portion with hyperkinetic basal segments. Atypical variants showing akinesia of the middle portion of the ventricle have also been documented.2 Stress cardiomyopathy commonly occurs in women over the age of 70 who have experienced physical or emotional stress, and generally resolves a few days after the initial presentation. The cause of this syndrome has not been described; nonetheless, recent studies have cited severe achalasia as a possible triggering event for stress cardiomyopathy.3 Clinically, the most common symptoms at presentation are chest pain or discomfort (63%-90%), or dyspnea (16%-24%). Stress cardiomyopathy is associated with electrocardiographic changes similar to those seen in acute coronary syndromes, specifically ST segment elevation (67%-75%) with troponin elevation in more than 70% and creatine kinase elevation in 56% of cases, as well as regional contraction alterations with no evidence of obstructive coronary disease.4 In this study we proposed to investigate whether there are differences in circadian and seasonal characteristics, symptoms at presentation, triggering events, and diagnostic data related to stress cardiomyopathy in Hispanic patients as compared to non-Hispanic patients.
Following ethics committee approval, we reviewed the echocardiographic records from January 2005 to January 2009. Among the total, 67 patients with suspected stress cardiomyopathy were identified. We analyzed their demographic data, medical history, cardiac markers, 12-lead electrocardiography findings, echocardiography results, coronary angiography data, ventriculography results at the time of the event, and hospitalization records.
Selected patients had to meet the diagnostic criteria for stress cardiomyopathy established by the Mayo clinic: a) transient akinesia or dyskinesia of the left ventricular apex and middle segments with regional contraction abnormalities extending beyond a single epicardial vascular distribution; b) absence of obstructive coronary disease or angiographic evidence of atherosclerotic plaque rupture; c) new electrocardiographic abnormalities (i.e., ST segment elevation or T-wave inversion); and d) absence of recent head injury, intracranial bleeding, pheochromocytoma, obstructive epicardial coronary artery disease, myocarditis, or hypertrophic cardiomyopathy.
We excluded 17 patients with intermediate grade coronary disease (50%-70% stenosis in at least 1 epicardial coronary artery with a corresponding regional abnormality) and those with regional contraction abnormalities in which there was no resolution or echocardiographic follow-up had not been performed. Fifty patients with stress cardiomyopathy were analyzed, 23 Hispanic and 27 non-Hispanic.
To differentiate between Hispanic and non-Hispanic patients, we applied the ethnicity classification used in the 2010 population census of the United States. According to this system, individuals from Cuba, Puerto Rico, South America, Central America, or any other culture of Spanish origin are considered Hispanic, regardless of their race.
The event was considered to be diurnal if it occurred between 7:00 AM and 7:00 PM, and nocturnal if it occurred between 7:01 PM and 6:59 AM. The year was divided into 4 seasons based on the standards of the northern hemisphere, and events were assigned according to the month in which they occurred. The months of July to September were considered summer; October to December, autumn; January to March, winter; and April to June, spring. A P value of<.05 was considered significant.
There were no significant differences between the groups in symptoms at presentation, electrocardiographic abnormalities, troponin I concentrations, initial and follow-up ejection fraction, triggering events, or in-hospital mortality (Table 1).
Demographic Data, Symptoms at Presentation, Diagnostic Data, and Mortality.
| Hispanic (n=23) | Non-Hispanic (n=27) | P | 95%CI | |
| Sex | ||||
| Women | 14 (60.9) | 17 (63.0) | 1.0 | |
| Men | 9 (39.1) | 10 (37.0) | 1.0 | |
| Age, years | 74.3±11 | 73.4±12 | .9 | –7.76 to 8.31 |
| Symptoms | ||||
| Precordial pain | 7 (30.4) | 7 (25.9) | .7 | |
| Dyspnea | 12 (52.2) | 13 (48.1) | 1.0 | |
| Asymptomatic | 5 (21.7) | 6 (22.2) | 1.0 | |
| Electrocardiographic findings | ||||
| Abnormal | 22 (95.6) | 24 (88.9) | .6 | |
| ST segment elevation | 7 (30.4) | 3 (11.1) | .1 | |
| ST segment depression | 5 (21.7) | 4 (14.8) | .7 | |
| T wave inversion | 17 (73.9) | 19 (70.4) | 1.0 | |
| Troponin I | ||||
| Elevated | 22 (95.6) | 24 (88.9) | .6 | |
| Peak, ng/dL | 7.7±21 | 4.5±8.7 | .6 | –8.42 to 13.28 |
| Ejection fraction | ||||
| Initial, % | 30±10 | 30±9 | .9 | –7.0 to 6.17 |
| Final, % | 56±9 | 55±8.8 | .8 | –4.52 to 5.43 |
| Triggering event | ||||
| Emotional | 8 (34.8) | 10 (37.0) | .8 | |
| Physical | 13 (56.5) | 15 (55.6) | 1.0 | |
| Not determined | 2 (8.7) | 2 (7.4) | .6 | |
| Deaths | ||||
| Any cause | 2 (8.7) | 1 (3.7) | .6 | |
| Patients with recurrence | 1 (4.3) | 1 (3.7) | .6 | |
95%CI, 95% confidence interval.
The data are expressed as no. (%) or mean ± standard deviation.
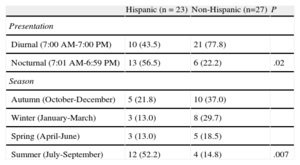
As to the time of day and frequency in the distinct seasons, some differences were found between Hispanic and non-Hispanic patients (Table 2). Stress cardiomyopathy occurred more frequently in the summer months in Hispanic than in non-Hispanic patients. Hispanics may respond differently to high temperatures; nonetheless, other studies are needed to prove or exclude this theory.
Circadian and Seasonal Distribution of Stress Cardiomyopathy in Hispanic and non-Hispanic Patients.
| Hispanic (n=23) | Non-Hispanic (n=27) | P | |
| Presentation | |||
| Diurnal (7:00 AM-7:00 PM) | 10 (43.5) | 21 (77.8) | |
| Nocturnal (7:01 AM-6:59 PM) | 13 (56.5) | 6 (22.2) | .02 |
| Season | |||
| Autumn (October-December) | 5 (21.8) | 10 (37.0) | |
| Winter (January-March) | 3 (13.0) | 8 (29.7) | |
| Spring (April-June) | 3 (13.0) | 5 (18.5) | |
| Summer (July-September) | 12 (52.2) | 4 (14.8) | .007 |
The data are expressed as no. (%).
We also found a higher incidence of stress cardiomyopathy during the night hours in Hispanic patients, which contrasts with the known incidence of acute myocardial infarction during the morning hours.5 The clear difference with respect to the circadian peaks of myocardial infarction could hypothetically emphasize the physiopathological differences between the 2 conditions.
The prognosis is generally favorable. In-hospital mortality ranges from 1%-8%.6 In the Hispanic group, we found a complete improvement of the ejection fraction, but slightly higher in-hospital mortality. The 2 deaths that occurred in Hispanic patients were secondary to non-cardiac causes (sepsis), which indicates that stress cardiomyopathy, in itself, is related to deteriorated health status rather than being a cause of death.