Brucella is one of the most important zoonotic infections worldwide caused by the intracellular Gram-negative bacteria Brucella, which is transmitted to humans either through contaminated food or via direct contact with infected animals.1Brucella endocarditis (BE) is one of the most feared complication of brucellosis today since it can be life-threatening.
Brucella is endemic in animals and humans within the Middle East region, including Lebanon. Of note, the fifth largest world outbreak of Brucella occurred in Lebanon beginning in 2017 with a total of 1180 cases.2 According to the World Health Organization Eastern Mediterranean Regional Office (EMRO), the annual incidence of brucellosis in Lebanon was between 3.5 and 9 cases per 100 000 inhabitants from 1997 to October 2009.3 Due to its endemicity, it is common in clinical practice in Lebanon to include brucellosis in the differential diagnosis when working up a patient with fever of unknown origin.
There are only a few case reports in the literature about BE due to infrequent recognition of the disease. The organism appears to have a predilection for invading damaged endocardial tissue and tends to cause aortic and mitral valve endocarditis.4 While some case reports describe BE involving the mitral and aortic valves, cases of BE involving the pulmonary valve are exceedingly rare in the literature. We herein present such a case.
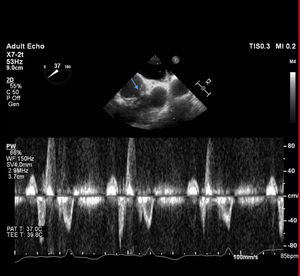
A 41-year-old woman presented to the clinic for a 1-month history of intermittent fever reaching 39°C and occasional cough. She also complained of fatigue and persistent nausea during the last month. Her past medical history was significant for Tetralogy of Fallot, for which she underwent 2 surgical corrections at 3 and 9 years of age. She also had pulmonary valve replacement and patch repair of her ventricular septal defect 10 years previously. She denied any exposure to pets or intravenous drug use. At her initial presentation, all her vital signs, including temperature, were within the reference range. Physical examination did not yield any significant findings except a systolic ejection murmur on the left sternal border. Initial blood tests revealed mild leukopenia with a white blood cell count (WBC) of 3300/cu.mm (reference range 4000-11 000/cu.mm) and mildly elevated transaminase enzymes (serum glutamic-oxaloacetic transaminase of 62 units/L and serum glutamic pyruvic transaminase of 57 units/L). The patient also had elevated lactate dehydrogenase of 288 units/L. C-reactive protein and erythrocyte sedimentation rate were elevated at values of 29.6mg/L and 50mm/h, respectively. Brucella serology was ordered and both direct and indirect titers were positive at 1:320. She was therefore treated with doxycycline and trimethoprim-sulfamethoxazole for 6 weeks and improved significantly. However, 2 months later, her symptoms recurred. Blood culture was positive for Brucella and antibody titers were unchanged. Transthoracic echocardiography showed severe right ventricular dilation and 2 masses consistent with vegetations on the pulmonary valve, the larger of the 2 measuring 12mm in length. Transesophageal echocardiography showed moderate regurgitation of the pulmonary valve prosthesis with accompanying vegetations and no abscess, in addition to the presence of a hypermobile oscillating mass in the pulmonary artery with no evidence of abscess formation (figure 1). All the other valves were normal.
.")
Medical treatment was initiated and the patient was started on streptomycin 1g intramuscularly daily, doxycycline 100mg orally twice daily, and rifampin 600mg orally daily. Six weeks after treatment, the patient showed mild symptom improvement. The rifampin dose was increased to 900mg daily and, 2 months later, she showed with almost complete symptom resolution with only mild residual fatigue. The patient consented for the publication of the case.
The cases of BE described in the literature involve mainly the aortic or mitral valves, such as the case of brucellosis-related endocarditis and spondylitis due to Brucella melitensis biovar that was reported by Whuan Zhuan et al.4
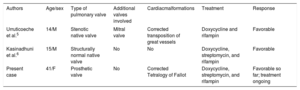
Only 2 cases of Brucella endocarditis of the pulmonary valve have been reported in the literature (table 1). The first was a 14-year-old patient who was treated for transposition of the great vessels and who had pulmonary valve stenosis with mitral insufficiency and was then diagnosed with BE involving both the pulmonic and mitral valves5. Kasinadhuni et al.6 also described a patient with BE involving a structurally normal pulmonary valve and without any predisposing factors such as intravenous drug abuse. As in our case, both patients were managed with medical treatment only. However, our case is unique in that it involves a prosthetic rather than a native pulmonary valve. The therapeutic regimen adopted for our patient was based on a World Health Organization recommendation that includes doxycycline plus an aminoglycoside alongside trimethoprim-sulfamethoxazole or rifampin for at least 8 weeks.
Summary of reported cases of Brucella endocarditis involving the pulmonary valve
| Authors | Age/sex | Type of pulmonary valve | Additional valves involved | Cardiacmalformations | Treatment | Response |
|---|---|---|---|---|---|---|
| Urruticoeche et al.5 | 14/M | Stenotic native valve | Mitral valve | Corrected transposition of great vessels | Doxycycline and rifampin | Favorable |
| Kasinadhuni et al.6 | 15/M | Structurally normal native valve | No | No | Doxycycline, streptomycin, and rifampin | Favorable |
| Present case | 41/F | Prosthetic valve | No | Corrected Tetralogy of Fallot | Doxycycline, streptomycin, and rifampin | Favorable so far; treatment ongoing |
None.
AUTHORS’ CONTRIBUTIONSAll authors contributed equally.
CONFLICTS OF INTERESTNone.
.