We read with interest the scientific letter by Couto Mallón et al.1 reporting a case of early outflow graft stenosis in a HeartWare (Medtronic, United States) left ventricular assist device (LVAD) diagnosed mainly because of an increase in hemolysis parameters and resolved with a percutaneous intervention with stenting.
We would like mention that the clinical presentation and management of an outflow graft obstruction may vary according to the etiology and type of LVAD. To illustrate the latter, we present the case of a 51-year-old woman with a prior history of hypertension, obesity, chronic obstructive pulmonary disease, and end-stage chronic heart failure due to ischemic cardiomyopathy admitted for cardiogenic shock. A HeartMate 3 LVAD (Abbott, United States) was implanted and the patient had an uneventful postoperative course.
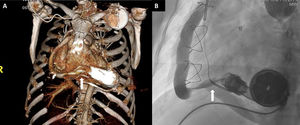
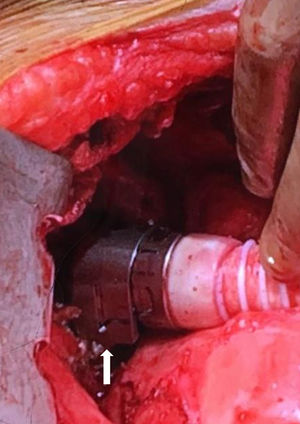
Two years later, she was admitted for new-onset low flow alarms. Her blood pressure was well controlled and laboratory tests were unremarkable with no signs of hemolysis. Transthoracic echocardiography showed severe left ventricular dilatation and severely decreased left ventricular ejection fraction. The aortic and mitral valves could not be assessed due to poor visualization. Hypovolemia was initially suspected, so diuretics were discontinued, and intravenous fluids were administered. A few days later, the patient was readmitted for persistence of low flow alarms, and now overt signs of congestive heart failure with shortness of breath were present. A right heart catheterization was performed. With a baseline speed of 5600rpm, the right atrial pressure was 13 mmHg, the pulmonary artery pressure was 45/27 mmHg with a mean of 33 mmHg, and the pulmonary capillary wedge pressure was 27 mmHg. Cardiac index was 2.18 lpm/m2. Despite a progressive increase of speed to 6800rpm, the pump was unable to unload the left ventricle and the pulmonary capillary wedge pressure remained at 26 mmHg. An outflow graft obstruction was suspected, and a chest computed tomography with 3-dimensional reconstruction was performed (figure 1A) and was suggestive of an outflow graft twist. The twist was confirmed by angiography with catheterization of the outflow graft from the ascending aorta (figure 1B and video 1 of the supplementary data). Surgical untwisting of the outflow graft in a clockwise direction was done without complications and a clip was placed to avoid a recurrence (figure 2). Pump flow immediately increased from 2.6 lpm to 5.2 lpm with a rapid improvement in hemodynamics. Intraoperative transesophageal echocardiography also showed a reduction in left ventricular size and mitral regurgitation. The aortic valve, which had opened with every beat, now remained closed (video 2 of the supplementary data).
. B: angiogram of the outflow graft confirming a twist in the last portion near the connection with the pump (arrow).")
 during the surgery to secure the swivel joint and prevent recurrences.")
Twisting of the outflow graft is a late complication appearing in 1.6% of patients supported with early iterations of the HeartMate 3 with a median time of 500 days after implantation.2 The mechanism behind the twist is a swivel joint connecting the pump with the outflow graft, designed to allow rotation during implantation to ensure a correct placement of the graft. However, it is believed that, in some cases, cardiothoracic movements are transmitted to the pump causing an insidious rotation of the graft leading to a complete twist with significant outflow graft obstruction, which can manifest as persistent low flow alarms. In addition, thrombosis can occur as a result of the twist and lead to a rise in lactate dehydrogenase levels. Of importance, although thrombosis must always be in the differential diagnosis of pump malfunction, this complication is less common in HeartMate 3 than in other types of LVAD. In fact, in the MOMENTUM trial, thrombosis was suspected in 7 of the 515 implants and was confirmed in only 2 of them.3 After a careful clinical assessment including laboratory tests, echocardiography and sometimes an invasive hemodynamic ramp test, when pump malfunction is suspected chest computed tomography is recommended to assess the integrity of the outflow graft.2 Once the twist is diagnosed, the preferred treatment is surgery with manual untwisting of the graft followed by a clip placement to avoid rotation of the swivel joint. Minimally invasive surgical techniques have been also described4 but due to the nature of the obstruction, it is uncertain if percutaneous approaches can be successful. A clip to secure the swivel joint has been available since the end of 2018 and should be placed during implantation to prevent this complication.5
FUNDINGM. Rivas-Lasarte received a Magda Heras mobility grant from the Spanish Society of Cardiology.
CONFLICTS OF INTERESTD.J. Goldstein is an educator and surgical proctor for Abbott and National PI for the MOMENTUM 3 trial. U.P. Jorde is a consultant for Abbott.
Supplementary data associated with this article can be found in the online version available at https://doi.org/10.1016/j.rec.2020.09.008