We present an exceptional case of Wolff-Parkinson-White syndrome associated with a right-sided accessory pathway (AP) at the level of a fistula between the right atrial appendage and right ventricle.
A 16-year-old patient with a history of palpitations with Wolff-Parkinson-White syndrome was referred for ablation (Figure 1A). There were no findings of structural heart disease on echocardiogram. A first electrophysiologic study confirmed a right-sided AP with a minimum RR interval in atrial fibrillation 200ms and retrograde conduction via the AP with retrograde atrial activity earlier in the lateral tricuspid annulus. Several radiofrequency applications at this level failed to eliminate conduction. A second procedure failed despite a sheath being used to improve stability. For this reason, the patient was referred to another hospital. In the third electrophysiological study, the earliest atrioventricular activity was detected at the level of the right atrial appendage (Figure 1B). A new ablation procedure using an irrigated-tip radiofrequency catheter was unsuccessful. It was then suspected that the AP had an epicardial insertion originating in the right atrial appendage. For this reason, cardiac computed tomography angiography was performed that showed a slightly dilated right atrium with an abnormal tubular-shaped connection between the right atrial appendage and the lateral basal portion of the right ventricle (Figure 2A). All other cardiac structures were normal. Given this finding, and after 3 unsuccessful endocardial ablation procedures, it was decided to refer the patient to another hospital with experience in treating arrhythmias in pediatric patients with minimally invasive surgery.1 The right chest cavity was entered via 3 small incisions in the submammary sulcus. This procedure was followed by video-assisted thoracoscopy and epicardial cryoablation of the AP in the tricuspid annulus (Figure 2B and Figure 2C). AP conduction was immediately eliminated. The patient was discharged from hospital at 48hours with good prognosis.

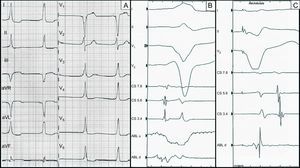
A: electrogram prior to ablation. B: endocavitary recording in sinus rhythm, with the ablation catheter located in the right atrial appendage. The atrioventricular interval is very short at this level. Monopolar recording shows QS pattern. C: endocavitary recording with ventricular pacing. The ablation catheter is again located in the right atrial appendage. A very short ventriculoatrial interval can be seen at this level.
. B: surgical image showing the fistula after pericardiotomy (arrow). C: epicardial cryoablation (arrow).")
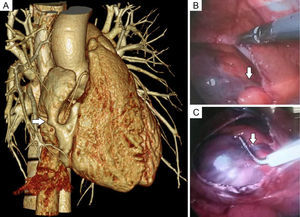
A: 3-dimensional reconstruction of computed tomography angiography showing the fistula connecting the right atrial appendage with the basal portion of the right ventricle (arrow). B: surgical image showing the fistula after pericardiotomy (arrow). C: epicardial cryoablation (arrow).
The typical location for APs is in the endocardium close to the atrioventricular ring. The atrial or ventricular insertion is sometimes further away from this site. Less often, the location is epicardial and exceptionally involves cardiac abnormalities such as diverticulum or right atrial appendage fistula.2–5
Endocavitary catheter ablation is highly effective. Difficulties in ablation are associated with subsequent relapse. Three elements associated with difficulties in AP ablation have been described in the literature: atypical location, erroneous location of the insertion site, and technical difficulties in achieving ablation. In these situations, the combination of new electroanatomic mapping, x-ray mapping, and x-ray imaging techniques can be of immense help in correct diagnosis and treatment2,5,6 which, in some cases, must be surgical. The surgical treatment of AP is well established and its usefulness has been proven. However, percutaneous ablation has confined the surgical approach to complex cases with mainly epicardial location.
We can see how the diagnosis and ablation of an AP can sometimes be a complex task. Imaging techniques such as cardiac computed tomography angiography can be very useful and should probably be performed more frequently, especially after failure of the initial approach. These techniques provide anatomical data that help in detecting and predicting difficulties in ablation procedures and thus in rethinking the approach. If surgery is needed, it is important to bear in mind the minimally invasive approach as a safe and effective option with excellent esthetic results (Figure of the supplementary material).
The authors would like to thank rest of the team for their collaboration, especially Dr Basterra, Dr Martínez, and Dr Romero for their invaluable help.