
Keywords
INTRODUCTION
Ergotamine is an ergot alkaloid used to prevent vascular headaches such as migraine or cluster headache. Its prolonged or excessive use should be avoided due to the risk of ergotism, gangrene, or becoming dependent on the drug.
Due to its vasoconstrictive effect it can reduce cerebral flow, precipitate angina, produce myocardial infarction, or aggravate an intermittent claudication. However, its effect on heart valves is less well known. We now describe 2 cases of valvular heart disease.
Case 1
A 30-year-old male was sent to us from the gastrointestinal unit, where he was under study due to a painful hepatomegaly, because chest x-ray revealed cardiomegaly. He had no history of heart disease or rheumatic fever. For the last 10 years he had been using 2-mg ergotamine suppositories prophylactically twice a day (Hemicraneal®) for his headaches. During physical exploration, auscultation revealed a pansystolic murmur in the mitral area, and a painful hepatomegaly was found that resolved upon starting diuretic treatment.
The electrocardiogram showed P mitrale, and echocardiography demonstrated valvular and subvalvular enlargement of the mitral valve with severe failure and moderate failure of the tricuspid valve. Left ventricular function was preserved and diameters were within the upper limit of normality (ejection fraction, 58%; left ventricle diameter, 57 mm).
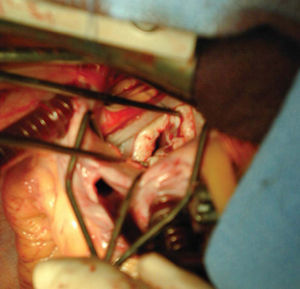
Given the patient's age, we tried to save the valves and carried out a commissurotomy and Cosgrove ring annuloplasty in the mitral and bicuspid position. Macroscopic examination revealed a white, opaque and indurated swelling in the valve and atrium (Figure 1); microscopic examination revealed a myofibroblastic subendothelial swelling (Figure 2). Despite presenting minimal failure, the patient came back a few months later with severe mitral failure requiring the implantation of a mechanical prosthesis (Carbomedics). After 2 years of follow-up, the patient remains asymptomatic and has abandoned the use of ergotamines.

Figure 1. Intraoperative image of the mitral valve.

Figure 2. Under the endocardial surface (to the left of the photograph) there is a layer of myofibroblasts arranged in parallel on a matrix of mucopolysaccharides with some elastic and collagen fibers that have not destroyed the tissue architecture nor presented associated signs of inflammation. To the left of the photograph a column of myocytes from the subjacent myocardium can be seen. Muscle-specific actin, Dako R, 1:5.
Case 2
This involves a 49-year-old woman with a personal history of psychiatric disease and chronic use of 2-4 mg of ergotamine per day during the last 15 years to control her headaches. She was admitted to hospital 10 years before for ergotamine-induced vasculopathy that started with subacute ischemia in the legs and arteriographic stenosis of both popliteal cavities. A moderate double mitral injury was found under echocardiographic follow-up. Despite this, the patient continued to take ergotamine and did not attend cardiographic follow-ups.
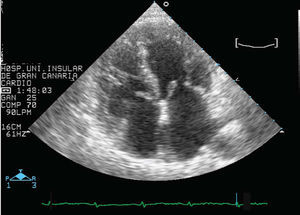
She is currently under the care of the psychiatric service which requested an evaluation as the patient presented dyspnea at mild exertion. Echocardiographic examination revealed multiple valve disease (Figure 3) with severe mitral stenosis, moderate mitral failure, and moderate-severe aortic, tricuspid and pulmonary valve failure, with preserved left ventricular function (ejection fraction 60%, left ventricle diameter 55 mm) and persistent sinus rhythm.

Figure 3. Echocardiography along the apical axis, where mitral and tricuspid valve swelling is evident.
Due to the findings and the functional degree of the patient, surgery was proposed which she rejected. The need to completely abandon the use of ergotamines was emphasized.
DISCUSSION
Ergotamine-induced valvular heart disease is a little known disorder due to the ever-decreasing use of these drugs to control migraine, tending only to appear with chronic and excessive use and is an infrequent complication.
The 2 cases presented refer to patients with valvular heart disease due to chronic use of ergotamine, histologically demonstrated to be the causative agent in the first case. In the second case, the absence of a background of rheumatic fever, the chronic and excessive use of ergotic drugs and multiple valve disease led us toward this diagnostic possibility, although the final and definitive diagnosis is anatomicopathological1-3; whenever possible the treatment of choice is surgery to preserve the valves.4,5
Thus, it is important to auscultate patients who use ergotamine chronically6 and, if there is a murmur, treatment should be discontinued and echocardiographic control implemented.
Correspondence: Dr. E. Martínez Quintana.
Alcalde Ramírez Bethencourt, 10 3-A. 35003 Las Palmas de Gran Canaria. España.
E-mail: efrenmq@eresmas.com