Keywords
INTRODUCTION
Fistulas between the aorta and cardiac cavities are rare and usually found in the right cavities. The presence of fistulas between the aorta and the left atrium (AOF-LA) is associated with complications of infectious endocarditis1 and paravalvular abscess, aortic dissection,2 and surgery affecting the valve or aortic root. We describe a patient with LA-AOF after resection of a left atrial myxoma presenting heart failure who underwent percutaneous treatment with an Amplatzer device for closure of interventricular communication.
CLINICAL CASE
Woman, 72 years old, admitted to hospital due to heart failure. She had undergone intervention in another center on two occasions for left atrial myxoma and posterior relapse (18 years and 15 years before, respectively) and had been diagnosed at follow-up with asymptomatic LA-AOF. Electrocardiogram showed atrial flutter that was electrically cardioverted. The patient continued with heart failure despite treatment with diuretics and captopril. Transesophageal echocardiogram showed LA-AOF through the noncoronary sinus with an important shunt through it. The left ventricle was mildly dilated and presented preserved systolic function.
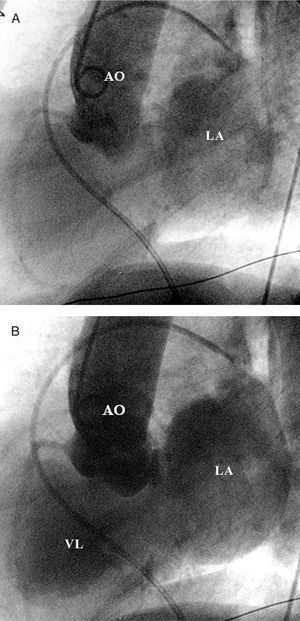
Cardiac catheterization was done showing normal lung pressure (30/14/20) and a pulmonary capillary pressure of 14 mm Hg. Aortography showed a large flow of contrast agent from the noncoronary sinus to the left atrium (Figure 1A and B).

Figure 1. A: fistula between the noncoronary sinus of the aorta and left atrium. Aortography in lateral projection (90° LAO); only the aorta and left atrium are filled in these initial images. B: finally, the aorta, atrium, and left ventricle are contrast-filled. LA indicates left atrium; AO, aorta; LV, left ventricle.
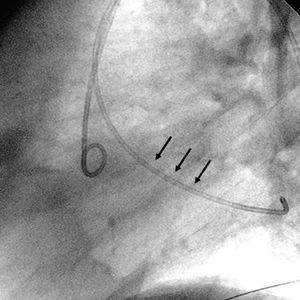
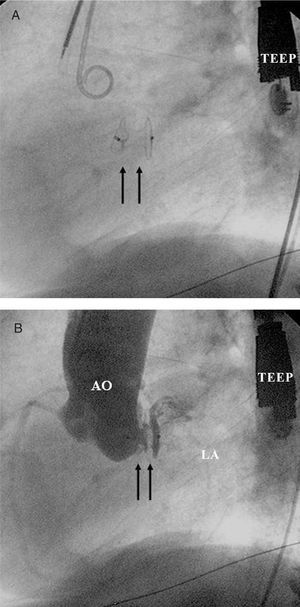
We decided on transcutaneous closure of the LA-AOF which was done via the right femoral artery. By use of a right coronary Judkins catheter, a hydrophilic guidewire was advanced from the aorta, via the fistula, to the left atrium with the catheter over this (Figure 2). Next, a long high-support guidewire was introduced into the left atrium and the coronary right catheter was exchanged for an Amplatzer delivery system. Through this system, an Amplatzer device was advanced via this system to close the 12-mm interventricular communication (AGA Medical Corporation, Golden Valley, Minneapolis, USA). This device is made of nitinol mesh with dacron patches inside consisting of 2 disks joined by a 7-mm central neck. Under fluoroscopic guidance and transesophageal echocardiogram, the delivery system was gradually withdrawn until the device was completely deployed, leaving 1 disc in the left atrium and the other in the aorta, checking that valve operation was not blocked. Transesophageal echocardiogram and control aortography showed that the device had been correctly placed with minimum leakage to the left atrium (Figure 3A and B). The patient received 100 mg aspirin/day to which 75 mg clopidogrel/day was added for 3 months. At 6-month follow-up, the patient was asymptomatic and the echocardiogram did not show residual shunt.

Figure 2. Passage of the catheter (arrows) from the aorta through the fistula to the left atrium.

Figure 3. A: Amplatzer device (arrows) in the fistula under fluoroscopic guidance. B: aortography after implantation of the Amplatzer device in the fistula with minimum residual leak. LA indicates left atrium; AO, aorta. TEEP, transesophageal echocardiography probe.
DISCUSSION
Closure of LA-AOF is indicated in symptomatic patients and surgery is the standard treatment. Transcutaneous closure was based on the favorable angiographic characteristics (noncoronary sinus, small diameter) and the background of 2 heart operations.
Recently, isolated experiences have been reported with an Amplatzer device in the treatment of perivalvar leak involving prosthetic mitral valve,3 sinus rupture of Valsalva aneurysm in right cavities,4 aortopulmonary window,5 and coronary fistulas in right cavities.6
Closure of LA-AOF with an Amplatzer device for anterograde closure of the ductus has been described in the literature with subsequent closure of an ostium secundum-type interatrial communication.7 Not having to carry out transeptal puncture would have suggested the anterograde approach to the authors making it possible for them to implant a device for ductus closure (with a single external disc that remains in the aorta). We chose the retrograde approach due to its simplicity aiming to implant an interventricular communication closure device.
Choice of the device was based on angiographic and echocardiographic findings, and the need for two discs to be anchored in the aorta and left atrium with a 7-mm central neck.
The 80-cm length of the Amplatzer delivery system makes a brachial approach necessary, but in short patients, as in this case, a femoral approach was possible. Potential risks could involve occluding a coronary ostium or restricting the movement of the aortic valves. In the present case, the fistula was located in the noncoronary sinus and had a small diameter, meaning that there was less risk, but such possible complications should be assessed before definitively releasing the device.
In conclusion, the percutaneous closure of LA-AOF with an Amplatzer-type device can be considered a therapeutic option in cases when the anatomy is favorable.
Correspondence: Dr. J.M. Hernández García.
Unidad del Corazón. Hemodinámica. Hospital Universitario Virgen de la Victoria.
Campus Teatinos, s/n. 29010 Málaga. España.
E-mail: jmhg@secardiologia.es