Septal coronary branches arising from the right coronary artery (RCA) or the right coronary sinus, known as descending septal artery (DSA)1 or Bonapace's branch,2 have rarely been described. However, the DSA might play an important role in certain situations, highlighting the need for its proper identification and evaluation. The present series reviews 3 cases of DSA identified during coronary angiography in different clinical scenarios.
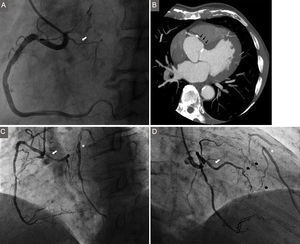
A 60-year-old man was referred for coronary angiography due to exertional chest pain and a significant lesion in the RCA detected by coronary computed tomography angiography. Through the right femoral artery, a multipurpose catheter was used to cannulate the RCA. A DSA emerging from a common ostium with the RCA was visualized (Figure 1A). The RCA lesion was successfully stented.
. B: Coronary computed tomography angiography performed in the same patient. A poorly defined descending septal artery is observed (black arrows). C and D: Left anterior oblique 60° and right anterior oblique 30° right coronary artery projections with a significant lesion in its mid-segment. A descending septal artery originating from the proximal segment (type I, white arrows) provides collaterals to a chronically occluded left anterior descending (asterisk) through several septal branches (black arrows).")
A: Left anterior oblique 60° projection of the right coronary artery. White arrow: descending septal artery sharing a common ostium with the right coronary artery (type II). B: Coronary computed tomography angiography performed in the same patient. A poorly defined descending septal artery is observed (black arrows). C and D: Left anterior oblique 60° and right anterior oblique 30° right coronary artery projections with a significant lesion in its mid-segment. A descending septal artery originating from the proximal segment (type I, white arrows) provides collaterals to a chronically occluded left anterior descending (asterisk) through several septal branches (black arrows).
A 68 year-old man was admitted with a non-ST-segment elevation myocardial infarction. Via the right radial artery, the RCA was catheterized with a Judkins right catheter. A DSA arising from the proximal segment was detected, providing collateral circulation to the left anterior descending (LAD) artery through several septal branches (Figures 1C-1D). Angiography of the left coronary artery confirmed the chronic occlusion of the LAD. The patient was referred for coronary artery bypass surgery.
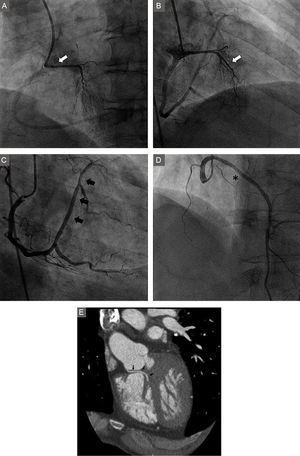
Finally, in a 56 year-old man referred for coronary angiography because of heart failure and poor left ventricular ejection fraction, a DSA independently originated from the right coronary sinus was accidentally cannulated (Figures 2A-2B) while attempting to localize the RCA with a Judkins right catheter via the right radial artery. The RCA had a normal origin. The posterolateral branch of the RCA continued toward the atrioventricular groove giving marginal branches (Figure 2C), thus replacing an orthotopic circumflex artery. An ectopic LAD arising from the right coronary sinus (Figure 2D) was identified. No significant lesions were detected.
. C: Right coronary artery angiography. The posterolateral branch continues toward the atrioventricular groove forming the circumflex artery (black arrows). D: Ectopic left anterior descending, with absence of the first septal branch (asterisk). E: Coronary computed tomography angiography showing a well-defined independent descending septal artery.")
A and B: Selective contrast injections in a descending septal artery independently originating at the right aortic sinus (type IV, white arrow). C: Right coronary artery angiography. The posterolateral branch continues toward the atrioventricular groove forming the circumflex artery (black arrows). D: Ectopic left anterior descending, with absence of the first septal branch (asterisk). E: Coronary computed tomography angiography showing a well-defined independent descending septal artery.
Available information about DSA arises from post-mortem studies, which report an incidence varying from 12% to 85%.2 This contrasts with its extremely infrequent identification in clinical practice. This difference could be explained by the higher perfusion pressures used and the absence of vascular tone in post-mortem specimens.2 Furthermore, the position of the catheter a few millimeters distal to the RCA ostium during coronary angiography can easily mask this branch.
The DSA can arise from up to 4 different locations and the anatomical variant originating from the first centimeter of the RCA is the most frequent.1 In an attempt to homogenize the angiographic description of the DSA, we propose to define as type I those variants emerging within the proximal segment of the RCA; type II as those sharing a common ostium with the RCA; type III as those sharing an ostium with the conal branch and type IV as those arising independently from the right coronary sinus.
The DSA provides blood supply to the posterobasal aspect of the interventricular septum, the atrioventricular node, and the His bundle. In the presence of coronary artery disease, its role as a source of collateral circulation has been recognized.1,2 These anastomoses are mainly connected with other septal branches3
The DSA can rarely be part of a combined coronary artery anomaly. The third case presented is extremely rare and, to the best of our knowledge, no similar coronary anomaly has been described. The DSA can be of interest even in patients with hypertrophic cardiomyopathy. Kurita et al4 performed a percutaneous septal alcohol ablation through a DSA, preceded by the demonstration of its contribution to the perfusion of the basal interventricular septum.
Technical aspects concerning the evaluation of the DSA should be addressed. A relatively deep cannulation of the RCA may prevent its identification. A DSA arising from an independent ostium is mostly accidentally identified while attempting to find the RCA. Contrast back-flow during injections in the RCA might reveal its presence. Nonselective contrast injections in the right coronary sinus could be used when a DSA is strongly suspected, especially in the absence of a well-developed first septal branch in the LAD. Multipurpose or Amplatz right catheters might be useful to selectively engage the DSA. The role of noninvasive techniques in evaluating DSA seems to be limited. The trajectory and the small caliber of this vessel could hamper its delimitation (Figures 1B and 2E).
DSA is an infrequent finding during coronary angiography that can be of interest in specific scenarios. Operators should be aware of its existence and perform a careful evaluation particularly in those situations in which a DSA might have therapeutic implications.