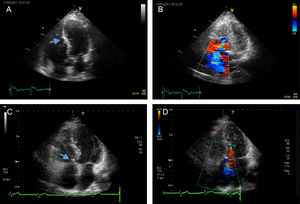

We present 3 cases of Ebstein anomaly and severe tricuspid regurgitation treated with cone reconstruction as described by da Silva et al.1 The patients were 13, 17, and 56 years old and weighed 51, 58, and 92kg, respectively. Briefly, the operation was performed through median sternotomy and extracorporeal circulation via aortic and bicaval cannulation, with antegrade cardioplegia for myocardial protection. On opening the right atrium, we observed apical displacement of the posterior and septal leaflets (Figure A) causing severe insufficiency (Figure B) with atrialization of the ventricular wall. All 3 patients underwent partial (almost complete) mobilization of the tricuspid valve, extensive delamination of the subvalvular apparatus, and longitudinal plication of the free wall of the right ventricle (segment corresponding to the posterior leaflet). The cone of the tricuspid valve was reconstructed (with clockwise rotation) to create a new commissure and the valve was reattached to its true annulus (Figure C). In line with current recommendations,2 prophylactic ablation of the cavotricuspid isthmus was performed in the 56-year-old patient (Figure of the supplementary material). Good results were observed after a follow-up of 38, 18, and 6 months respectively (Figure D); the patients had good functional class without medication (Table) and were in sinus rhythm. All the patients have consented to their data being reported.
. B, Severe tricuspid regurgitation. C, Postoperative image showing tricuspid valve reinserted in the true annulus (arrow). D, Postoperative image showing mild tricuspidregurgitation.")
Data for the 3 Patients in the Current Series and Comparison With the Series Described by da Silva et al.1
| Age, y | Weight, kg | ECC, min | Clamping, min | CTI Ablation | Follow-up, mo | Functional Class | Tricuspid Insufficiency | |
|---|---|---|---|---|---|---|---|---|
| Case 1 | 13 | 51 | 125 | 80 | 38 | NYHA I | Mild | |
| Case 2 | 17 | 58 | 125 | 85 | 18 | NYHA I | Mild-moderate | |
| Case 3 | 56 | 92 | 114 | 82 | Yes | 6 | NYHA I | Mild |
| Da Silva et al.1 | 17 (1-49) | ? | 104 | 70 | 9/40 | 49 (3-143) | NYHA I | Mild |
Abbreviations: ECC, extracorporeal circulation; CTI, cavotricuspid isthmus; NYHA, New York Heart Association functional class.
The early work at the Mayo Clinic laid the foundations for the surgical correction of Ebstein anomaly.3 Since then, numerous authors have introduced modifications and new techniques,4,5 such as superior cavopulmonary anastomosis (ventricular and medial) and valve replacement. Carpentier et al.4 proposed longitudinal plication of the atrialized chamber of the right ventricle, modifying the transverse approach described by Danielson et al.3 and creating the basis for the procedure introduced by da Silva et al.1 These last authors modified the technique described by Carpentier et al. by creating a tricuspid or bicuspid valve instead of a monocuspid valve. They also proposed full coaptation between the valvular tissue with central blood flow rather than the off-center flow between the monocuspid leaflet and septum described by Carpentier et al.
The cone procedure published by da Silva et al.1 merged the best aspects of the classical techniques (eg, elimination of the atrialized ventricle, reduction of the tricuspid diameter, and reimplantation of the true annulus) and introduced new concepts such as “almost complete” mobilization of the tricuspid valve, and “delamination” of the subvalvular apparatus. It is precisely this last technique that permits the creation of a conical structure with the valve and the resulting subvalvular apparatus, which is key to the competence of the tricuspid valve.
The achievements of da Silva et al.1 led to the widespread adoption of their surgical technique and the practical disappearance of earlier ones. The technique has been standardized in different age groups, including neonates who showed poor results with earlier techniques or had been treated with single-ventricle surgery.5
One concern with the correction described by da Silva et al.1 is the risk of tricuspid stenosis due to the considerable reduction in valve diameter. However, follow-up of their patients showed no stenosis, even when the resulting diameter was smaller than that of the mitral valve. As a preventive measure, da Silva et al. recommended not implanting the annulus in the tricuspid position, particularly in young patients.
Wolff-Parkinson-White–type arrhythmias are common in patients with Ebstein anomaly. Of the 40 patients in the series reported by da Silva et al., 9 underwent ablation of anomalous pathways during surgical repair. The most recent guidelines recommend prophylactic ablation during surgery for adult patients.2
The surgical procedure for Ebstein anomaly is one of several new surgical techniques being introduced in Spain.6 Our initial experience is very limited, as we had only 3 cases over a period of 3 years. This frequency, however, is in line with rates described by other authors (mean of 1 case per year5). The technique is reproducible, as evidenced by the similarities in surgical times (Table). Our early results are promising, although we acknowledge that longer follow-up is needed. We consider that the central flow and full coaptation between valvular tissue achieved with the modification described by da Silva et al.1 may be key to the success of the technique. Finally, prophylactic ablation of the cavotricuspid isthmus is a simple and technique that can be recommended, particularly in adult patients.