Transcatheter aortic valve implantation (TAVI) is indicated in patients with severe aortic stenosis with an intermediate or high surgical risk or who are deemed inoperable.1,2 Transfemoral access is the most common route, but is not always possible if the patient has peripheral vascular disease. Alternative routes have been proposed, not always with good associated outcomes.3 With transaxillary access, there is a shorter distance from the puncture of the aortic annulus, which potentially enhances control during implantation. The left axillary artery is used more often because it allows better coaxial alignment of the device and the aortic annulus, but it is more fragile than the common femoral artery and is noncompressible. The possibility of performing TAVI with a highly-flexible valve that can be advanced in tortuous arteries, such as the Portico (Abbott Vascular; Santa Clara, California, USA), with a sheathless introduction4 and therefore reduced diameter, could reduce vascular complications and allow its use in smaller arteries.
The clinical guidelines1 advocate a multidisciplinary Heart Team, although in reality the roles of the cardiac surgeon (CS) and interventional cardiologist (IC) vary, depending on the hospital.
The aim of our study was to describe our experience with the Portico self-expanding valve implanted using a sheathless technique via a transaxillary route, in which both the CS and the IC actively participated in decision-making before and during implantation.
We carried out a retrospective study with clinical follow-up. The primary objectives were the success of the intervention and the complication rate.
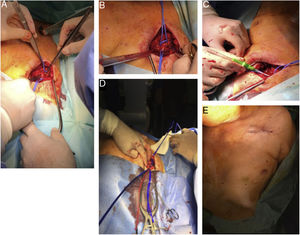
The study was conducted between March 2017 and December 2018. It included 29 patients with severe aortic stenosis who were being considered for TAVI but who had inadequate transfemoral access due to vessel diameter <6-6.5mm, calcification, or severe tortuosity, but feasible transaxillary access (vessel diameter> 5mm, absence of calcification and arterial tortuosity and an angle between the subclavian artery and the aorta of ≥ 60°). The procedure was conducted in a fully equipped operating room with 2 CSs and 2 ICs present. Under general anesthetic, a 4-6cm incision was made below and parallel to the left clavicle. The pectoralis major was dissected in the direction of its fibers, the clavipectoral fascia was opened and the pectoralis minor was exposed and retracted laterally. Taking special care of the brachial plexus, surgical cut-down exposed the axillary artery (figure 1A), which was sutured with a purse-string suture (figure 1B). The artery was punctured distal to the suture edge, and a 6-Fr sheath was introduced (figure 1C). An AL-1 diagnostic catheter was then advanced across the aortic valve, and a Safari extra support guidewire was introduced. The 6-Fr sheath was changed to a 14-Fr sheath. Aortic valvuloplasty was performed in indicated cases, the sheath was removed, and the Portico valve was introduced directly without a sheath over the Safari guidewire (figure 1D). Valve implantation was performed according to standard procedures. If postdilatation was required, the delivery system was changed for the 14-Fr sheath. When the valve had been implanted, and after ensuring hemostasis, the surgical wound was closed (figure 1E).

A: cut-down to expose the right axillary artery. B: purse-string suture of the axillary artery. C: 6-Fr sheath in the axillary artery after puncture. D: Portico valve in the axillary artery delivered without a sheath, using an extra support guidewire. E: closure of the surgical wound.
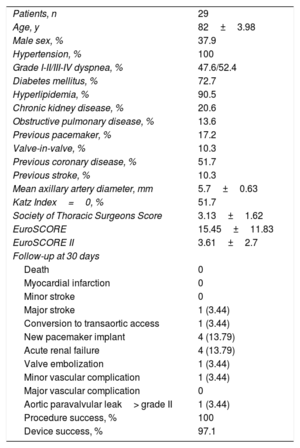
The patients’ characteristics at baseline and follow-up at 30 days are shown in table 1.
Characteristics at baseline and 30-day follow-up
| Patients, n | 29 |
| Age, y | 82±3.98 |
| Male sex, % | 37.9 |
| Hypertension, % | 100 |
| Grade I-II/III-IV dyspnea, % | 47.6/52.4 |
| Diabetes mellitus, % | 72.7 |
| Hyperlipidemia, % | 90.5 |
| Chronic kidney disease, % | 20.6 |
| Obstructive pulmonary disease, % | 13.6 |
| Previous pacemaker, % | 17.2 |
| Valve-in-valve, % | 10.3 |
| Previous coronary disease, % | 51.7 |
| Previous stroke, % | 10.3 |
| Mean axillary artery diameter, mm | 5.7±0.63 |
| Katz Index=0, % | 51.7 |
| Society of Thoracic Surgeons Score | 3.13±1.62 |
| EuroSCORE | 15.45±11.83 |
| EuroSCORE II | 3.61±2.7 |
| Follow-up at 30 days | |
| Death | 0 |
| Myocardial infarction | 0 |
| Minor stroke | 0 |
| Major stroke | 1 (3.44) |
| Conversion to transaortic access | 1 (3.44) |
| New pacemaker implant | 4 (13.79) |
| Acute renal failure | 4 (13.79) |
| Valve embolization | 1 (3.44) |
| Minor vascular complication | 1 (3.44) |
| Major vascular complication | 0 |
| Aortic paravalvular leak> grade II | 1 (3.44) |
| Procedure success, % | 100 |
| Device success, % | 97.1 |
This is the largest series in the literature and describes our experience with TAVI using sheathless implantation of the Portico valve via transaxillary access, with the active participation of both CSs and ICs. A series on sheathless implantation of the Portico system via transfemoral access has been published,5 with outcomes similar to ours, but our patients were somewhat more complex, as they were not suitable for femoral access. Our data demonstrate that this is a safe procedure, with very few vascular complications, with only 1 case of arterial dissection without compromised flow and with conversion to transaortic access. This is relevant because the patients in this series had an axillary artery diameter smaller than that recommended for the standard Portico technique (6mm), and as the procedure was performed without a sheath, it was possible to implant the valve via smaller arteries (as small as 5mm or even slightly less if there was no arterial calcification). For this procedure, a good study of the axillary artery, a good surgical technique and experience in the implantation of this valve are essential.
A series on fully percutaneous transaxillary access has also been published.6 This requires a very precise use of the closure devices and a protection guidewire; use of a surgical technique simplifies this. Stenting was still performed in a considerable number of cases (11%), with 2% requiring vascular reintervention that would be avoided or solved quickly with surgical access.
In conclusion, our series indicates that sheathless implantation of the self-expanding Portico valve is feasible and safe when there is a good previous study of the axillary artery and good surgical technique that reduces the risk of vascular complications. In addition, it allows the procedure to be performed in arteries of <6mm diameter, thus broadening the scope of the types of patients who may be offered this procedure. Furthermore, the presence of the CS during the procedure allows rapid action to be taken should any potentially fatal complications arise.
CONFLICTS OF INTERESTJ.F. Díaz Fernández is a proctor for the Portico valve.
.