Persistent left superior vena cava is the most common variant of systemic venous drainage, with an incidence of 0.3% to 0.5% in the general population and of 3% to 10% in patients with congenital heart disease.1 This anomaly arises when obliteration of the left anterior cardinal vein, which drains into the right atrium via the coronary sinus, fails to occur. Dilation of the coronary sinus constitutes the main echocardiographic sign leading to suspicion of its presence. It is usually an incidental finding and, in recent years, is frequently diagnosed during the prenatal period. It is generally an isolated entity, but there have been reports of a higher incidence of associated cardiac and extracardiac anomalies, while its presence is related to the development of obstructive lesions of the left heart.2
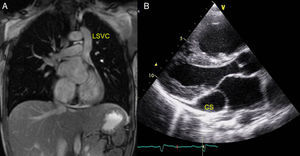
Persistent left superior vena cava in the absence of right superior vena cava (Figure A) is a less common anomaly and is caused by the obliteration, during embryogenesis, of the right anterior cardinal vein with persistence of the left anterior cardinal vein. Its incidence is 0.09% to 0.13% among patients with congenital heart defects, and only isolated cases have been reported in the literature. The largest series consists of 9 cases and a review of the literature.3 This anomaly is associated with congenital heart defects in 46% of the patients and with rhythm disorders in 36%.3–5

In a review of our database from March 1995 to July 2015, we found 150 pediatric patients (aged 0-18 years) with persistent left superior vena cava; of these, the right vena cava was absent in 12 (8%). The characteristics of these patients are shown in the Table. There were 7 boys and 5 girls. The diagnosis was made during a prenatal study in 6 patients (50%), during a postnatal study in the context of an associated heart defect in 4 (33.3%), and during an echocardiographic study for another purpose (innocent murmur and examination of a newborn in whom sepsis was suspected) in 2 (16.6%). In our series, 7 patients (58%) had an associated heart defect: atrial septal defect in 4 (57%), tetralogy of Fallot in 2 (28.5%), and coarctation of the aorta in 1 (14.2%). The remaining 5 (42%) had structurally normal hearts. In addition, 2 patients (1 with no heart defect and the other with an atrial septal defect) had severe pulmonary hypertension of the newborn. The 6 patients with a prenatal diagnosis included 4 (66.6%) with smaller-than-expected left heart chambers and aortic arch; of these, 3 had no associated heart defect and they showed a progressive normalization after birth, and the fourth had tetralogy of Fallot. With regard to rhythm disorders, 4 patients (33.3%) had ectopic atrial rhythm, and no episodes of ventricular or supraventricular tachycardia were observed. Extracardiac malformations were found in 6 patients (50%) as follows: multiple malformation syndrome in 4 (33.3%) (Table), hypoacusis and psychomotor retardation of unknown origin in 1 (8%), and Down syndrome in 1 (8%). The remaining 6 (50%) had normal phenotypes and karyotypes.
Characteristics of the 12 Patients
| Patients | Sex | Age at diagnosis, mo | Heart defect/treated surgically | ECG | Extracardiac anomaly | PHT | Outcome/cause of death |
|---|---|---|---|---|---|---|---|
| 1 | G | 2 | - | SR | - | - | Asymptomatic |
| 2 | B | 60 | AC/yes | EAR | - | - | Asymptomatic |
| 3 | G | PD | ASD/yes | EAR | MR | - | Asymptomatic |
| 4 | B | 0 | TF/yes | EAR | MMSa | - | Death/postop |
| 5 | B | 1 | ASD/yes | SR | DS | - | Asymptomatic |
| 6 | G | 0 | - | SR | MMSb | Yes | Death/PHT |
| 7 | B | PD | - | EAR | - | - | Asymptomatic |
| 8 | G | PD | - | SR | - | - | Asymptomatic |
| 9 | B | PD | TF/yes | SR | MMSc | - | Death/postop |
| 10 | B | PD | - | SR | - | - | Asymptomatic |
| 11 | G | PD | ASD/no | SR | MMSd | Yes | Death/PHT |
| 12 | B | 192 | ASD/yes | SR | - | - | Asymptomatic |
AC, aortic coarctation; ASD, atrial septal defect; B, boy; DS, Down syndrome; EAR, ectopic atrial rhythm; ECG, electrocardiogram; G, girl; MMS, multiple malformation syndrome; MR, mental retardation; PD, prenatal diagnosis; PHT, pulmonary hypertension; postop, postoperative; SR, sinus rhythm; TF, tetralogy of Fallot.
The 4 (33%) patients who died during follow-up had a multiple malformation syndrome. Two died after a pulmonary hypertensive crisis, 1 of them had an atrial septal defect and died prior to surgery, and the other had a structurally normal heart. The other 2 nonsurvivors had tetralogy of Fallot; 1 died after corrective surgery and the other after reintervention for severe pulmonary insufficiency. The 8 survivors (66.6%) remain asymptomatic.
In the 4 patients with atrial septal defects, there was marked dilation of the right heart chambers, and 2 of them required corrective surgery at an earlier than usual age (8 months and 2 years). The patients with tetralogy of Fallot underwent intervention with the customary timing (before the age of 6 months).
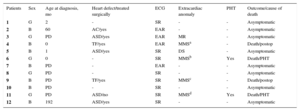
This report involves the largest series of patients with persistent left superior vena cava in the absence of right superior vena cava of all those published to date. In conclusion, this is a very uncommon anomaly, for which intrauterine diagnosis is possible; its frequent association with cardiac and extracardiac malformations, as well as with multiple malformation syndromes, necessitates a complete study in the fetus, including genetic analysis. The severe dilation of the coronary sinus (as shown in Figure B) and the resulting distortion of the mitral annulus could have an intrauterine effect on left ventricular filling, which would explain its frequent association with small left heart chambers and with other left-sided obstructive lesions. In patients with atrial septal defect, the compression of the mitral annulus could favor a greater left-to-right shunt through the defect, which would explain the marked dilation of the right heart chambers and the need for early surgical correction. In our series, the patients with no other anomalies had an asymptomatic course, with postnatal normalization of the size of the left heart chambers. Thus, we consider that the high mortality rate observed in the series was probably related to the presence of other associated malformations.