Keywords
INTRODUCTION
Congenital coronary artery anomalies are an uncommon angiographic finding (0.2%-1.4%).1 One of the rarest of these variants is single coronary artery (0.026%),1 in which the entire coronary system originates from a single coronary ostium.2 In most cases, single coronary artery is an incidental finding on coronary angiography and has no clinical repercussions; nonetheless, it can cause angina, myocardial infarction, or even sudden death.3
In this article we describe the clinical and angiographic characteristics of 3 patients with single coronary artery and associated atherosclerotic disease, who were evaluated for symptoms of myocardial ischemia.
METHODS
The cases described in this article were seen in our hospital between September 2007 and January 2009. In all 3 patients, the diagnosis was based on findings obtained with coronary angiography and 64-slice multidetector computed tomography (MDCT).
RESULTS
From a total of 4324 diagnostic coronary angiographies performed in our center in the time period mentioned above, 35 coronary artery anomalies of any type were diagnosed (0.8%); 3 of them (0.06%) were single coronary arteries. The clinical and angiographic characteristics of the 3 patients with this condition are described as follows and are presented in Table 1.

Patient 1
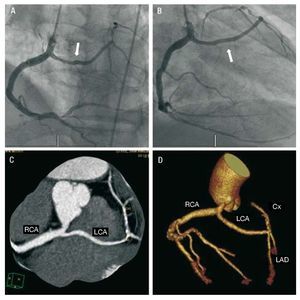
A 50-year-old man, smoker, with hypercholesterolemia, was admitted to our hospital for acute myocardial infarction in a lateral location. He underwent fibrinolysis and presented criteria for reperfusion. Coronary angiography showed a single coronary artery originating in the right sinus of Valsalva; after a short course, the artery divided into its 2 right and left branches. The right coronary artery (RCA) was a highly developed vessel with a stenosis in the ostium of the posterolateral (PL) branch. The left coronary artery (LCA), after a long course, divided into the left anterior descending (LAD) artery and the circumflex (Cx) artery, which presented various severe stenoses in the proximal third. MDCT study confirmed the coronary angiography findings and showed a long intramuscular portion of the LCA that reached the anterior interventricular groove (Figure 1). Based on these findings, percutaneous transluminal coronary angioplasty (PTCA) was carried out, with implantation of a drug-eluting stent in the PL branch. In a second surgical stage, the Cx lesions were treated by placement of 2 drug-eluting stents.

Figure 1. Patient 1. A: coronary angiography in a left anterior oblique view; the left coronary artery (LCA) arises from the proximal segment of the right coronary artery (arrow) and a severe lesion is seen in the ostium of the posterolateral branch. B: coronary angiography in a right anterior oblique view; the LCA shows a long course before it divides (arrow). C and D: multidetector computed tomography curved multiplanar reformatted image (C) and 3-dimensional volume-rendered reconstructed image of the coronary system used for stereotaxis magnetic navigation (D). Cx indicates circumflex artery; LAD, left anterior descending artery; LCA, left coronary artery; RCA, right coronary artery.
Patient 2
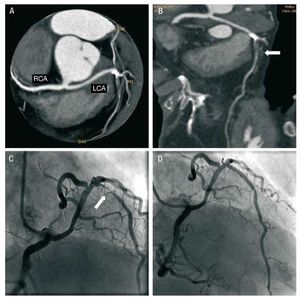
A 78-year-old woman with hypertrophic cardiomyopathy was hospitalized for recurrent episodes of precordial oppression and dyspnea. The exercise stress test findings were inconclusive. MDCT revealed a single coronary artery originating in the right sinus of Valsalva; the vessel divided into its 2 right and left branches after a short course. The LCA had a long intramuscular course and then divided into the Cx and LAD, which presented a severe proximal stenosis and a large calcification (Figure 2). Coronary angiography confirmed the MDCT findings, and PTCA was performed, with implantation of a drug-eluting stent in the LAD.

Figure 2. Patient 2. A and B: images obtained with multidetector computed tomography and processed with curved multiplanar reformatting (A) and planar reformatting (B) showing the origin of the single coronary artery in the right sinus of Valsalva; the left anterior descending artery (LAD) presents a severe calcified lesion in the proximal segment (arrows). C: coronary angiography in a right anterior oblique view showing the severe lesion in the proximal LAD (arrow). D: outcome following angioplasty. LCA indicates left coronary artery; RCA, right coronary artery.
Patient 3
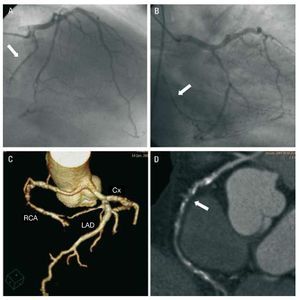
A 62-year-old man, smoker, with hypercholesterolemia and type 2 diabetes, had a history of non-Q-wave acute myocardial infarction for which a drug-eluting stent was implanted in the proximal LAD. In the preoperative workup, an anomalous origin of the RCA, arising from the LCA, was detected. In addition, the RCA presented an apparently chronic occlusion in the middle segment.
On this occasion, the patient was consulting for angina of various months' duration occurring with considerable exertion. Stress testing was clinically and electrically positive. Coronary angiography showed severe stenosis in the proximal segment of the Cx, whereas the LAD stent remained patent. MDCT study confirmed the coronary angiography findings. The RCA ran anterior to the aorta and presented a long occlusion (15 mm) and calcification (Figure 3). A new drug-eluting stent was placed in the Cx, and the posterior clinical course was satisfactory.

Figure 3. Patient 3. A: coronary angiography in a cranial right anterior oblique view (RAO); the right coronary artery (RCA) arises from the left coronary trunk and is occluded in the middle segment (arrow). B: coronary angiography in a caudal RAO view showing distal RCA filling by collateral circulation (arrow); the circumflex artery presents a severe stenosis in the proximal segment, before the origin of the first marginal. C: multidetector computed tomography with 3-dimensional reconstruction and volume rendering of the coronary system. D: curved multiplanar reconstruction showing calcified occlusion of the RCA (arrow). Cx indicates circumflex artery; LAD, left anterior descending artery; RCA, right coronary artery.
DISCUSSION
The prognosis of single coronary artery is not well defined. In some cases, myocardial perfusion can be affected, leading to signs of ischemia, heart failure or even sudden death; the condition should be suspected when cardiac events occur in young persons.3 The ischemia can be caused by abrupt angulation of the vessel or by compression as it runs between the great vessels, usually in association with heavy physical exertion. In patients in whom the single coronary divides distally, a long sequence of serial resistances can occur, leading to ischemia without significant lesions.4 Four possible courses of the LCA have been described when it arises from the RCA: septal, anterior free wall, retroaortic, and interarterial. Among them, only the interarterial course (between the aorta and pulmonary artery) implies a poor prognosis, per se.5 When the RCA arises from the LCA, there are 2 possible configurations, an anterior or an interarterial (retroaortic) course, the latter implying higher risk.6
It is evident that these patients can also have atherosclerotic lesions. Because the cause of the symptoms in our 3 patients was the atherosclerotic coronary disease and not the anomaly itself, the clinical presentation was different in each case. None of these patients had a coronary artery running between the aorta and pulmonary artery, and all were older; these facts confer a prognosis similar to that of any other patient with ischemic heart disease.
Therapy should be individualized depending on the ischemic symptoms, the presence of associated coronary lesions, and the patient's age. When the symptoms of myocardial ischemia appear after the age of 50, the incidence of sudden death is very low and the therapeutic approach to follow is similar to that used in the remaining patient population with ischemic heart disease. In young patients with a variant having an interarterial course, however, the risk of sudden death is higher and the therapeutic approach should be aggressive, with surgery being the treatment of choice.7
Usually, the first examination carried out to investigate symptoms of suspected coronary origin is exercise stress testing. If the coronary anomalies are substantial, however, this test can be negative. For this reason, a comprehensive anatomic study is recommended when a congenital coronary anomaly is suspected, particularly in young patients because of their higher risk of sudden death. Coronary angiography is the technique commonly used to detect congenital anomalies of the coronary arteries, although catheterization may be technically difficult in some cases. Failed visualization of a coronary artery should alert the operator to a possible anomalous origin of the vessel. In patients in whom angiographic diagnosis is difficult, other imaging techniques (eg, MDCT) may be useful to better define the coronary anatomy.8 This test is not justified when the diagnosis and therapeutic approach is clearly established by coronary angiography. MDCT is of special interest to exclude an arterial course between the pulmonary artery and the aorta, which has important clinical implications (risk of sudden death) and therapeutic implications (surgical approach). In 40.8% of cases in the Spanish Registry of Congenital Coronary Artery Anomalies Originating in the Contralateral Sinus of Valsalva (Registro de Anomalías Congénitas de las Arterias Coronarias con Origen en el Seno de Valsalva Contralateral, RACES) registry (23 300 coronary angiographies), the course of the anomalous coronary artery in relation to the great vessels was unknown, perhaps because additional imaging techniques were rarely used (only 2 cases, by transesophageal echocardiography and magnetic resonance imaging, respectively).1
Correspondence: Dr. J. A. de Agustín.
Unidad de Imagen Cardiovascular. Hospital Clínico San Carlos. Prof. Martín Lagos, s/n. 28040 Madrid. España.
E-mail: albertutor@hotmail.com
Received April 1, 2009.
Accepted for publication June 24, 2009.