Keywords
INTRODUCTION
Acute aortic dissection is associated with a very high mortality rate and usually represents a medical emergency.1,2 The association between chronic aortic dissection and fever has been known for years, but very few studies have related fever with acute aortic dissection. It therefore commonly goes unmentioned as a clinical manifestation of the condition in guidelines. A number of studies have proposed theories regarding the pathophysiology of inflammatory fever in acute aortic dissection.3,4 However, none has defined the clinical criteria in such patients that would allow an appropriate early diagnosis to be made. Fever has normally been described in the context of chronic aortic dissection.5
METHODS
This retrospective study, which covers a period of 10 years, was performed at the Hospital Universitario 12 de Octubre in Madrid. Patients were recruited using the diagnoses recorded in their discharge papers. All aortic lesions visible in imaging tests were deemed to represent an aortic dissection. Fever was deemed present when patient body temperature was ≥37.8°C.
The variables recorded in the present work were sex, age, whether the temperature was taken in the emergency room (yes/no), type of dissection according to the Stanford6 classification (A/B), the time elapsed between the beginning of the patient's condition and emergency attention being received, patient temperature in the emergency room, daily minimum and maximum body temperature, and the variation in daily body temperature (calculated by obtaining the mean differences between the daily maximum and minimum). The study did not identify patients with an intramural hematoma or symptomatic aortic ulcer (belonging to the most recent classification of acute aortic syndrome).6
All patients with fever were identified and decisions made regarding whether this was due to the dissection; the criteria for inflammatory fever were thus established (defined in Results). Among these patients the following data were noted: analytical abnormalities (leukocytosis >10 000/µL, neutrophilia >70%, lactate dehydrogenase), chest x-ray results, blood, urine, sputum and intravenous catheter culture results, and fever etiology (infectious, medication-induced, post-surgical, inflammatory, or other).
RESULTS
The studied cohort was composed of 59 patients, all with acute aortic dissection (43 [72%] men). The mean age was 60.3 (14.4) years. Forty-seven patients (79%) suffered a type A dissection, and 12 (21%) a type B dissection.
Body temperature had been taken in the emergency room in just 47.46% of patients (28/59), and the following distribution was noted: 22/28 (78.56%) patients were non-febrile, 3/28 (10.72%) had febricula, and 3/28 (10.72%) had fever. All patients had their temperature taken, however, within the first six hours of their hospital arrival. Six died in the first 24 h and 43 underwent surgery (41 with a type A dissection, 2 with a type B dissection).
Five patients of the cohort showed a condition compatible with fever secondary to acute aortic dissection (Table1). In these patients fever appeared within the first 48 h of the onset of symptoms. The duration of fever in those who did not undergo surgery or in whom diagnosis was delayed, was over 15 days. In these patients the maximum daily temperature was ≥37.8°C in more than 50% of measurements taken, and ≥37°C in 90% of measurements. The mean daily variation in the temperature of the 5 patients with inflammatory fever secondary to acute aortic dissection was 0.77 (0.3), 0.73 (0.39), 0.58 (0.28), 0.57 (0.3), and 0.81 (0.25)°C. The variation was <1.2°C in 85% of all measurements recorded.

Five patients presented with fever secondary to an infection (Table 1). The mean daily temperature variation in these patients during the febrile episode was 1.5 (0.7), 1.6 (0.6), 2 (0.8), 1.9 (1.1), and 3.1 (1.4)°C respectively. All 5 became afebrile with antibiotic treatment.
The difference in the mean variation of fever between patients with fever secondary to aortic dissection and those with fever of infectious etiology was significant (P=.015; 95%CI, 0.33-2.32).
According to the physicians' comments recorded in the examined medical histories, the patients with fever secondary to aortic dissection always showed a 'good general condition.' Chest x-rays showed nothing significant, except in one patient who was seen to have a pleural hemorrhage in the left hemithorax.
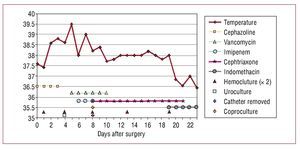
The 5 patients in whom fever was retrospectively attributed to their acute aortic dissection had all been subjected to multiple microbiological culture analyses. No results of microbiological interest were returned for four of these patients. The fifth was treated for bacteremia caused by Staphylococcus aureus secondary to a catheter infection some time after the fever secondary to the aortic dissection. During the febrile episode attributable to aortic dissection, four patients received different combinations of empiric, wide spectrum antibiotic treatment, despite which their fever remained for more than 2 weeks. In 3 of these 5 patients inflammatory fever secondary to aortic dissection was suspected, and in 2 of these 3 treatment with indomethacin was begun and antibiotic treatment suspended; fever remitted in these patients. Figure shows the abrupt disappearance of fever with the start of indomethacin treatment in 1 patient who had received different antibiotic treatments for 19 days.

Figure 1. Rapid remission of fever secondary to acute aortic dissection after beginning of indomethacin treatment following 19 days of varied antibiotic treatment.
DISCUSSION
Papers discussing series of patients with aortic dissection fail to mention fever as an associated manifestation7,8; in fact, even the International Registry of Acute Aortic Dissection9 fails to make any mention of this.
This careful, retrospective study of a series of patients with acute aortic dissection allowed the characteristics that discriminate between fever owed to a dissection itself and that owed to an intercurrent infectious process to be identified. The comparison of these groups allowed the identification of 2 patients whose fever was secondary to their acute aortic dissection, but for whom this diagnosis had not been made. Fever secondary to acute aortic dissection was mostly seen in patients with a type B dissection, a situation in which surgery is usually deferred. Fever begins between 48 and 72 h after the dissection occurs and microbiological tests are negative. The variation in body temperature in this kind of fever is significantly less than that caused by infection, and patients show a 'good general condition' during times when fever is apparent. The last of these clinical data has a very subjective interpretation, but it was repeatedly mentioned in the patients' reports. Fever rapidly disappears (in under 24 h) after beginning anti-inflammatory treatment (especially with indomethacin). When the diagnosis is uncertain, it might be reasonable to try a "therapeutic trial" with anti-inflammatory drugs while empirical anti-microbial treatment is maintained.
Only one paper has been published on inflammatory fever in a cohort of patients with acute aortic dissection,4 and it was concluded that a significant relationship existed between the size of the thrombus in the false lumen of the dissection and the duration of inflammatory fever. It should be noted, however, that the methods used involved no objective criteria for defining inflammatory fever secondary to dissection.
Based on the results of the present work, criteria for the diagnosis and treatment of fever secondary to acute aortic dissection are proposed (Table 2).

In conclusion, in subjects with acute aortic dissection there are a number of clinical data that allow one to distinguish between a fever secondary to the dissection itself and a process caused by an intercurrent infection. Their distinction may avoid the undertaking of certain complementary tests, reduce the duration of unnecessary antibiotic treatment, and avoid delay in embarking upon treatment that the patient might need for his/her aortic condition.
Francisco López-Medrano was the recipient of a research grant from the Fundación Mutua Madrileña.
Correspondence: Dr. F. López-Medrano.
Unidad de Enfermedades Infecciosas. Hospital Universitario 12 de Octubre.
Avda. Córdoba, s/n. 28041 Madrid. España.
E-mail: flmedrano@yahoo.es
Received February 3, 2009.
Accepted for publication June 24, 2009.