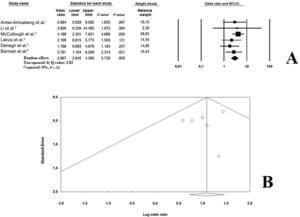
Recent analyses have demonstrated that COVID-19 patients with pre-existing cardiovascular risks and/or comorbidities have a higher risk of death in the short-term. However, the prognostic role of right bundle branch block (RBBB) in these patients has not yet been evaluated. The aim of this study was to perform a brief meta-analysis on the prognostic impact of RBBB on short-term mortality in COVID-19 patients. The study was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. The MEDLINE and Scopus databases were systematically searched for articles, published in English, from the inception of the COVID-19 pandemic (January 2020) through 1 May 2021 using the following Medical Subject Heading (MESH) terms: “COVID-19” AND “Arrhythmias” OR “Right bundle branch block”. Inclusion criteria were: a) studies enrolling participants with a confirmed diagnosis of COVID-19; b) providing data on the presence/absence of RBBB among survivors (S) and nonsurvivors (NS), allowing us to calculate an unadjusted odds ratio (OR) when not provided; and c) reporting all-cause mortality by the presence or absence or RBBB. We excluded case reports, review articles, editorials/letters, and case series with less than 10 participants, randomized controlled trials and studies including duplicate populations and investigations evaluating the electrocardiographic consequences of specific COVID-19 therapy. References from the included studies were screened to potentially identify other investigations meeting the inclusion criteria. Ethical approval and informed consent were not required as the study did not directly enrol human participants. The quality of the included studies was graded using the Newcastle-Ottawa quality assessment scale (NOS). Mortality risk data were pooled using the Mantel-Haenszel random effects models with odds ratios (OR) as the effect measure with 95% confidence intervals (CI). Heterogeneity among studies was assessed using Higgins and Thompson I2 statistic where I2 values correspond to the following levels of heterogeneity: low (< 25%), moderate (25%-75%) and high (> 75%). The presence of potential publication bias was verified by visual inspection of the funnel plot. Due to the low number of included studies (< 10), small-study bias was not examined as our analysis was underpowered to detect such bias. A predefined sensitivity analysis (leave-one-out analysis) was performed removing 1 study at a time, to evaluate the stability of our results. All meta-analyses were conducted using Comprehensive Meta-Analysis software, version 3 (Biostat, United States). The initial search resulted in 2049 articles (951 in PubMed and 1098 in Scopus, respectively). After we removed duplicates (n=885) and applied our inclusion criteria, 6 studies,1–6 enrolling 1904 patients (mean age 64.7 years old, 1176 males) were included in the analysis. All the investigations were of high quality according to the NOS. The most frequent comorbidities were arterial hypertension and diabetes mellitus. Conversely, the prevalence of heart failure, coronary artery disease and chronic obstructive pulmonary disease were not systematically reported in the reviewed investigations, making a comprehensive evaluation impossible (table 1). The mortality rate was 17.0% (n=324). RBBB was present in 150 COVID-19 participants (7.8% of cases). On pooled analysis, RBBB was significantly associated with a higher risk of death in the short-term (OR, 2.96; 95%CI, 2.04-4.30; P ≤ .0001; I2=0%) (figure 1A). Visual inspection of the relative funnel plot revealed no significant evidence of publication bias (figure 1B). Sensitivity analysis slightly changed the combined OR, which remained statistically significant across a range from 2.38 (95%CI,1.48-3.84) to 3.24 (95%CI, 2.16-4.85), suggesting that no single study had an undue impact on the study outcome. The results of present analysis suggest a higher mortality risk in COVID-19 patients with RBBB. We decided to analyze the impact on RBBB since several analyses have demonstrated that right ventricular dysfunction is frequently observed in COVID-19 patients and is associated with a poor prognosis.1,6 Because RBBB is an electrocardiographic sign of right ventricular strain and considering that right ventricular dysfunction is generally due to pulmonary microembolic events in COVID-19 patients, we hypothesized that this conduction disturbance may be related to a worst prognosis. However, we cannot exclude the possibility that those patients with more severe infection most frequently had RBBB.
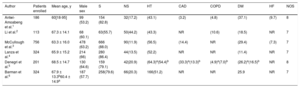
General characteristics of the patients enrolled
| Author | Patients enrolled | Mean age, y | Male sex | S | NS | HT | CAD | COPD | DM | HF | NOS |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Antwi-Amoabeng et al.1 | 186 | 60[18-95] | 99 (53.2) | 154 (82.8) | 32(17.2) | (43.1) | (3.2) | (4.8) | (37.1) | (9.7) | 8 |
| Li et al.2 | 113 | 67.3 ± 14.1 | 68 (60.1) | 63(55.7) | 50(44.2) | (43.3) | NR | (10.6) | (18.5) | NR | 7 |
| McCullough et al.3 | 756 | 63.3 ± 16.0 | 478 (63.2) | 666 (88.0) | 90(11.9) | (56.5) | (14.4) | NR | (29.4) | (7.3) | 7 |
| Lanza et al.4 | 324 | 65.9 ± 15.2 | 214 (66) | 280 (86.4) | 44(13.5) | (52.2) | NR | NR | (11.4) | NR | 7 |
| Denegri et al.5 | 201 | 68.5 ± 14.7 | 130 (64.6) | 159 (79.1) | 42(20.9) | (64.3)a(54.4)b | (33.3)a(13.3)b | (4.9)a(7.0)b | (26.2)a(16.5)b | NR | 8 |
| Barman et al.6 | 324 | 67.9 ± 13.3b60.4 ± 14.9a | 187 (57.7) | 258(79.6) | 66(20.3) | 166(51.2) | NR | NR | 25.9 | NR | 7 |
CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; DM, diabetes mellitus; HF, Heart failure; HT, arterial hypertension; NOS, Newcastle-Ottawa quality assessment scale; NS, nonsurvivors; S, Survivors.
Data are expressed as no. (%), mean ± standard deviation or median [interquartile range].

Unfortunately, we were unable to assess whether RBBB was already present before COVID-19 infection or whether it might be due to a secondary right ventricular overload caused by pulmonary micro- or macrothrombotic events, pre-existing pulmonary disease, or ventilatory support. Furthermore, none of the reviewed investigations made a distinction between complete and incomplete RBBB or for the setting of hospitalization (ie, intensive care unit or general wards). Moreover, the reported ORs were unadjusted for potential confounders and, despite the meta-regression performed, this aspect limited our final conclusions. Therefore, our results must be cautiously interpreted and considered preliminary. Further larger clinical studies are needed to confirm our preliminary results and to determine the potential pathophysiological mechanisms underlying this relationship.
FundingNone.
Authors’ contributionsM. Zuin: conception, draft, analysis, literature search; G. Rigatelli: draft, literature search, and analysis; L. Roncon: editing and literature search; G. Zuliani: editing and validation. All the authors have read and approved this manuscript.
Conflicts of interestNone of the authors have conflicts of interest to declare.