

Keywords
INTRODUCTION
Coronary collateral circulation usually appears when stable anterograde coronary blood flow is insufficient. It is frequently found in angiographic studies, generally associated with fixed atherosclerotic obstructions (partial or complete) of coronary arteries. Less common is the development of collateral circulation due to episodes of recurrent ischemia secondary to severe coronary vasospasm in coronary arteries without angiographically significant lesions. We present the case of a patient with a fixed moderate atherosclerotic lesion, associated with severe vasospasm and development of collateral circulation as a consequence of severe recurrent ischemia.
CLINICAL CASE
Our patient was a 51-year-old man, a heavy smoker with dyslipidemia, on dietary treatment but without other known cardiovascular risk factors. In recent months he had presented early morning effort angina which become progressively more frequent until it was a daily occurrence. The angina diminished with sublingual nitrates. Electrocardiogram (ECG) and baseline echocardiography results were normal. Clinical and electric treadmill testing results were positive (≤2 mm horizontal ST-segment depression) at 4 minutes of the Bruce protocol. A treatment regimen of aspirin and beta-blockers was established but no improvement in symptoms was observed. Baseline coronary angiography revealed a subocclusive lesion in the mediodistal right coronary artery (Figure 1), showing the distal vessel through herterocoronary collateral circulation (Figure 2). After bolus injection of nitroglycerin (3 0.2 mg bolus), the lesion was seen to reduce to moderate, its length diminished, and the distal vessel was normal in the anterograde injection (Figure 3). Following a later injection in the left coronary artery, collateral circulation was no longer visible. Subsequently, we started treatment with oral diltiazem and nitrates in transdermal patches, which improved the patient's symptoms.

Figure 1. Right coronary angiography in LAO 45-degree projection; long and severe mid-segment stenosis (arrows).

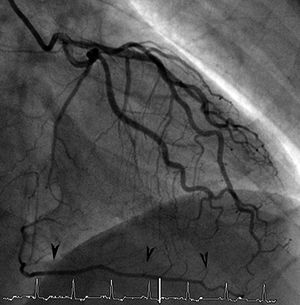
Figure 2. Left coronary angiography in RAO 30-degree projection. Descending posterior artery and distal right coronary artery can be seen due to heterocoronary collateral circulation arrows).

Figure 3. Right coronary angiography in lateral projection after repeated intracoronary administration of bolus of nitroglycerin. Focal moderate lesion in the mid-segment (arrow).
DISCUSSION
Coronary collateral circulation is the connection between different segments of the same artery or between different arteries that is established when the original blood flow is insufficient.1 It develops in response to intermittent myocardial ischemia,2 protects the myocardium and prevents ischemic events.3 Myocardial ischemia per se can induce development of collateral circulation, possibly thru biochemical signals that provoke the release of angiogenic growth factors.4 Collateral circulation can help protect the myocardium in patients with coronary artery disease, limits myocardial ischemia during coronary occlusion,5 and when well-developed can even minimize the infarction zone and predict presence of viable myocardium in patients with a history of previous infarction.6 This occurs more frequently in patients with severe fixed atherosclerotic coronary artery lesions (occlusions or subocclusions). It is less common to find well-established collateral circulation due to severe stenosis caused by coronary vasospasm. Development of transitory collateral circulation secondary to episodes of repeated coronary spasm, even in the absence of significant coronary artery lesions, has been reported.7-9
In vasospastic angina, the classic electrocardiogram pattern is of ST-segment elevation during ischemic episodes10. Presence of ST-segment depression in the ECG during episodes of angina due to coronary spasm can be put down to subendocardial ischemia caused by partial occlusion of an epicardial coronary artery and the transitory increase of blood flow provided by collateral circulation.11 According to Tada et al,12 this collateral circulation supplies blood flow thru preexisting vessels to ischemic regions during coronary spasm which prevents transmural ischemia, diminishes the degree of ischemia and is associated with ST-segment depression during episodes of angina. Yamagishi et al13 confirmed these findings reporting a lower frequency of ST-segment elevation during coronary spasm in patients with established collateral circulation.
Our patient demonstrated effort angina and ST-segment depression on treadmill testing. He had a moderate lesion in the right coronary artery associated with severe vasospasm that caused a subocclusive lesion. Our case highlights the need always to administer intracoronary bolus injection of nitroglycerin in diagnostic coronary angiography to determine the true severity of lesions. Our patient would probably be in "chronic spasm" and ischemia would be seen only on increasing the demand for oxygen during effort. The ST-segment depression in treadmill testing may be due to the lower degree of ischemia thanks to the blood flow contributed by the collateral circulation. Calcium antagonists and/or nitrates are the treatment of choice and were effective for our patient.
Correspondence: Dra. P. Sanz Mayordomo.
Budapest, 1. 28922 Alcorcón. Madrid. España.
E-mail: psanz@fhalcorcon.es