
To the Editor:
Digitalis intoxication is a frequent outcome of chronic treatment with digitalis glycosides but uncommon following accidental intake or self-poisoning.1 Ventricular arrhythmias are an expression of this complication and can usually be controlled thru conventional means including suspension of the drug. However, in the presence of potentially lethal arrhythmias and kidney failure difficult decisions must be taken as normal antiarrhythmic therapy may be inappropriate and put the patient at risk. In ventricular arrhythmia, bidirectional ventricular tachycardia (BVT) is a rare outcome; it is virtually a diagnosis of digitalis toxicity and indicates a life-threatening situation.
We present the case of a 75-year-old woman with antecedents of chronic atrial fibrillation and arterial hypertension, being treated with acenocoumarol, digoxin (0.25 mg/day) and lisinopril, who attended Emergency Room for dyspnea. In the initial physical examination we found tachypnea, jugular venous distension when reclined at 45 degrees, normotension and a poor general clinical status. In the cardiorespiratory examination, auscultation showed arrhythmic tones at 150 beats/minute and bibasal crepitations. Analysis showed urea 149 mg/dL, creatinine 3.1 mg/dL and potassium 5.1 mEq/L. The electrocardiogram (ECG) showed atrial fibrillation with a 150 beats/minute mean ventricular frequency (Figure 1). The patient was clinically stable following diuretic treatment and was hospitalized with improved renal function (urea, 130 mg/dL; creatinine, 2.6) and persistent hyperpotassemia (5.8 mEq/L). She maintained a regimen of 0.25 mg/day of oral digoxin until day 5 when she presented symptoms of left heart failure and hypotension (the ECG is in Figure 2). Frequency, regularity, and bidirectionality of the QRS complex in the frontal plane led us to diagnose BVT possibly caused by digitalis. Digoxinemia was 6 ng/mL (normal: 0.8-2 ng/mL). Given the potential life-threatening risk, disturbed ventricular rhythm in the presence of heart failure, kidney failure, hyperpotassemia, the fact that antiarrhythmic agents can entail increased risk and that electric cardioversion is counterindicated, we decided to use specific antidigoxin antibodies. After monitoring and a negative skin test, the patient was administered 450 mg of antidigoxin Fab with the altered rhythm disappearing within 1 hour of administration (Figure 3). Subsequent Doppler echocardiography showed concentric hypertrophy of the left ventricle with conserved systolic function.

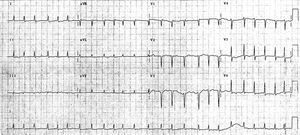
Figure 1. Atrial fibrillation with mean ventricular frequency 150 beats/minute. "Narrow" QRS complex, i.e. <120 ms duration.

Figure 2. Bidirectional ventricular tachycardia. Note that in the frontal plane QRS complex morphology alternates between 60° and +120°. Duration is <120 ms.

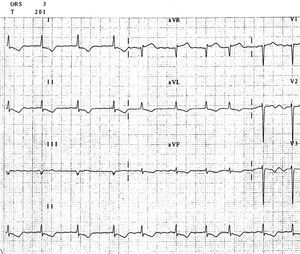
Figure 3. Atrial fibrillation with mean ventricular frequency 90 beats/minute. QRS complex morphology is again similar to that of QRS complex prior to ventricular tachycardia.
Administration of antidigoxin antibodies is a useful, safe alternative in the treatment of arrhythmias due to digitalis intoxication and hyperpotassemia, which is frequently associated with acute toxicity1 especially in life-threatening situations. Our patient presented BVT, an infrequent condition2 almost exclusively associated with digitalis intoxication. Bidirectional ventricular tachycardia is a polymorphic VT originating below the bundle of His bifurcation in which QRS complex morphology changes beat by beat. Although it has been related to effort- and/or emotion-induced sympathetic simulation linked to a cardiac ryonadine receptor gene (hRyR2) mutation,3 it is most frequently found in other pathologies associated with elevated sympathetic tone, as in digitalis intoxication or in hydroelectrolytic disturbances, especially in the presence of heart failure. It has an ominous prognosis due to possible degeneration to ventricular fibrillation and sudden death. In digitalis intoxication, Na/K pump block provokes increased automatism of the subsidiary pacemakers situated in some of the principal specific conduit system fascicles. Its involvement in impulse transmission means that in this type of ventricular tachycardia the QRS complex duration can be <120 ms; this contrasts with ventricular tachycardia originating in the Purkinje network or ventricular myocardium, when QRS complex duration is ≥120 ms.
Clinical use of antidigoxin Fab fragments was introduced in 1976 by Smith et al.4 It is generally agreed that they are effective and should be indicated in acute digitalis glycoside intoxication but no such consensus exists as to indications in intoxication during chronic treatment.5 The antiarrhythmic effect observed was especially relevant in our patient and avoided the risk associated with using antiarrhythmic agents and/or electric cardioversion in the presence of heart and kidney failure.6