Clinicians have a wealth of resources available to help them take existing evidence into account when making decisions. However, patients are the ones who actually have to live with the disease, so educating them should be a priority if they are to be able to adequately self-manage their condition. Clinical practice guidelines for some pathologies have made recommendations regarding patient education,1,2 but levels of patient knowledge are not all they should be.3 Our aim was to assess patients’ level of knowledge about their disease amongst those admitted to our unit.
We interviewed 100 randomly selected patients from those admitted to the cardiology department of our tertiary hospital in March 2012. Two cardiologists independently conducted verbal interviews using a pro-forma, closed-ended survey (Table 1). The study was blinded with regard to the physicians and nurses treating the patients interviewed. On admission, patients received information about their condition and the reason for admission. They also went through the nursing admission program and received written information on where they would be sent and details of their assigned physician (who visited and informed the patient daily), as well as receiving and completing informed consent forms. Subsequent statistical analysis was performed using SPSS/PC 17 (SPSS Inc., Chicago, Illiniois, United States). Continuous variables were expressed as means and confidence intervals, categorical variables as absolute numbers and percentages. Multivariate analysis was performed using binary logistic regression. Significance was set at P<.05.
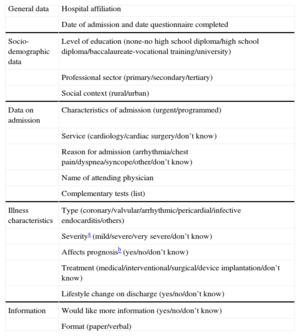
Survey Form Used, With Possible Response Options in Brackets
| General data | Hospital affiliation |
| Date of admission and date questionnaire completed | |
| Socio-demographic data | Level of education (none-no high school diploma/high school diploma/baccalaureate-vocational training/university) |
| Professional sector (primary/secondary/tertiary) | |
| Social context (rural/urban) | |
| Data on admission | Characteristics of admission (urgent/programmed) |
| Service (cardiology/cardiac surgery/don’t know) | |
| Reason for admission (arrhythmia/chest pain/dyspnea/syncope/other/don’t know) | |
| Name of attending physician | |
| Complementary tests (list) | |
| Illness characteristics | Type (coronary/valvular/arrhythmic/pericardial/infective endocarditis/others) |
| Severitya (mild/severe/very severe/don’t know) | |
| Affects prognosisb (yes/no/don’t know) | |
| Treatment (medical/interventional/surgical/device implantation/don’t know) | |
| Lifestyle change on discharge (yes/no/don’t know) | |
| Information | Would like more information (yes/no/don’t know) |
| Format (paper/verbal) |
Illnesses categorized as serious were acute myocardial infarction, coronary disease, ventricular arrhythmias, heart failure, infective endocarditis, severe valve disease, and ventricular dysfunction. Conditions categorized as very serious were hemodynamic instability, acute pulmonary edema, complicated endocarditis, resuscitated cardiac arrest.
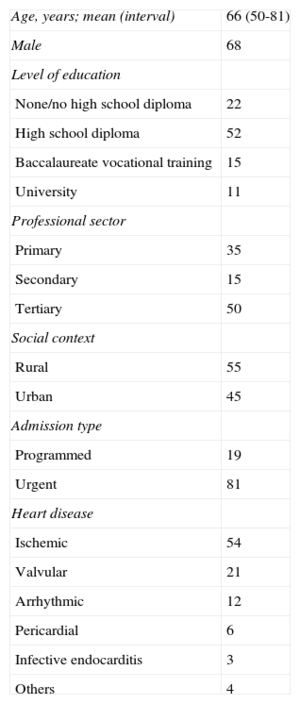
The study population's baseline characteristics are shown in Table 2. The median time-to-interview was day 3 [interquartile range, days 2-4]. Of those interviewed, 11% did not know the reason for their admission, 19% could not say which hospital service they were in, and 17% thought they had been admitted to cardiac surgery. Furthermore, 61% did not know their physician's name, 24% did not know what kind of heart disease they were experiencing, 32% could not provide information on the tests they had received, and 29% could not say what type of treatment they would be given. With regard to disease severity, 23% could not say how severe their disease was, 29% thought their disease was less severe than it actually was, and 22% were not sure whether the disease was relevant to their prognosis. Finally, 9% did not know whether they needed to make lifestyle changes after hospital discharge and 29.7% thought they would not make any changes even when changes were indicated for their condition.
Baseline Population Characteristics
| Age, years; mean (interval) | 66 (50-81) |
| Male | 68 |
| Level of education | |
| None/no high school diploma | 22 |
| High school diploma | 52 |
| Baccalaureate vocational training | 15 |
| University | 11 |
| Professional sector | |
| Primary | 35 |
| Secondary | 15 |
| Tertiary | 50 |
| Social context | |
| Rural | 55 |
| Urban | 45 |
| Admission type | |
| Programmed | 19 |
| Urgent | 81 |
| Heart disease | |
| Ischemic | 54 |
| Valvular | 21 |
| Arrhythmic | 12 |
| Pericardial | 6 |
| Infective endocarditis | 3 |
| Others | 4 |
Data are percentages unless otherwise indicated.
Multivariate analysis showed that lack of knowledge about the disease was associated with a low education level (no education or no high school diploma, odds ratio=5.78; 95% confidence interval, 1.14 to 29.87). Being female, older, working in the primary or secondary sectors, living in a rural area, or having undergone an emergency admission all trended toward association with less knowledge about the disease, although statistical significance was not reached.
Concerning information resources, 64% of respondents wanted more information about their disease, and 61% of these preferred to receive written information. Those who did not want information (36% of respondents, 100% male, mean age 59 years; medium-high educational level; tertiary sector workers; urban residence) had a high degree of knowledge, except as related to behavior modification (37.5% would not change, even though change was indicated).
It is difficult to draw definitive conclusions from this data, as we do not know what an optimal level of knowledge would be and there is a lack of supporting literature. Nevertheless, the study results do suggest that these patients have insufficient knowledge of their disease. Lower levels of self-care have been shown to be associated with poorer control of hypertension,4 while there is evidence that educational interventions can lead to improvements in knowledge about ischemic heart disease,5 in quality of life and number of readmissions in heart failure,2 and in quality of life, morbidity, and mortality in diabetes mellitus.1 On the other hand, analysis suggests that information available to patients online for conditions such as aortic aneurysm is of poor quality.6
Limitations of the present study include the relatively small number of patients included and that participants were from a single center. It remains to be seen whether these findings can be extrapolated to other centers. On a local level at least we have identified areas for improvement and subgroups, such as patients with lower educational levels, who could most benefit from further initiatives because this group showed the greatest lack of knowledge. As in diabetes mellitus, it is likely that the greatest benefit would come from programs tailored to patients’ age and sociocultural background.1
Investigating these aspects of patient management should form part of hospital quality programs and would help address information deficits in the physician-patient relationship.
.