The latest European Society of Cardiology and European Atherosclerosis Society guidelines for the management of dyslipidemias propose the definition of 4 levels of cardiovascular risk (very high, high, moderate, and low) to facilitate decision making and selection of the best therapeutic strategy.1
However, several studies indicate that different diagnostic and therapeutic approaches to cardiovascular risk (CVR) are used for women and men, both in primary and in secondary prevention; pharmacological undertreatment is common among women in secondary prevention or at high CVR, whereas there is a tendency to overtreat women at low CVR.2–4
The goal of this study was to evaluate the control of lipoprotein concentrations and the prescription of lipid-lowering drugs in the different stratification categories for CVR1; CVR was estimated using the calibrated Framingham function from the REGICOR study5 in participants aged ≥ 35 years (1170 women and 1042 men) in the HERMEX study, based in Extremadura, Spain.6 Participant parameters included history of risk factors and cardiovascular diseases, anthropometric measures, blood pressure, ankle brachial pressure index, medication with lipid-lowering drugs, and blood analyses. Data were analyzed with SPSS 22.0 for Windows. Significance of differences between mean values was calculated by Students’ t test, and between median values by the Mann–Whitney U test; significance of differences between proportions was calculated with the chi-square test or Fisher's exact test. Multivariable analysis was conducted by logistic regression, using the “Enter” method, with the dependent variable defined as achievement or nonachievement of the target values for low-density lipoprotein cholesterol (LDL-C) in the very high or high CVR categories. Independent variables included all those showing an association at P<.10 in the bivariable analysis and others associated in the literature with the use of lipid-lowering drugs, such as age, a history of smoking, obesity, diabetes mellitus, hypertension, peripheral artery disease, or chronic kidney disease.
The mean age of the study population was 53.3 years. Of the participants, 31.2% were smokers and 35.4% fulfilled the criteria for hypercholesterolemia; 48.5% of participants considered to be hypercholesterolemic were receiving treatment with lipid-lowering drugs (46.9% of men compared with 50.0% of women; P<.05) (Table 1).
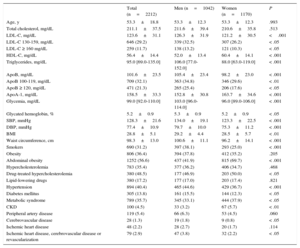
Principal Biological Parameters and Prevalence of Clinical Conditions
| Total (n=2212) | Men (n=1042) | Women (n=1170) | P | |
|---|---|---|---|---|
| Age, y | 53.3±18.8 | 53.3±12.3 | 53.3±12.3 | .993 |
| Total cholesterol, mg/dL | 211.1±37.5 | 211.6±39.4 | 210.6±35.8 | .513 |
| LDL-C, mg/dL | 123.6±31.1 | 126.3±31.9 | 121.2±30.5 | <.001 |
| LDL-C 130-159, mg/dL | 646 (29.2) | 339 (32.5) | 307 (26.2) | < .05 |
| LDL-C ≥ 160 mg/dL | 259 (11.7) | 138 (13.2) | 121 (10.3) | < .05 |
| HDL-C, mg/dL | 56.4±14.4 | 52.0±13.4 | 60.4±14.1 | < .001 |
| Triglycerides, mg/dL | 95.0 [69.0-135.0] | 106.0 [77.0-152.0] | 88.0 [63.0-119.0] | < .001 |
| ApoB, mg/dL | 101.6±23.5 | 105.4±23.4 | 98.2±23.0 | < .001 |
| ApoB 100-119, mg/dL | 709 (32.1) | 363 (34.8) | 346 (29.6) | < .01 |
| ApoB ≥ 120, mg/dL | 471 (21.3) | 265 (25.4) | 206 (17.6) | < .05 |
| ApoA-1, mg/dL | 158.5±33.3 | 152.8±30.8 | 163.7±34.6 | < .001 |
| Glycemia, mg/dL | 99.0 [92.0-110.0] | 103.0 [96.0-114.0] | 96.0 [89.0-106.0] | < .001 |
| Glycated hemoglobin, % | 5.2±0.9 | 5.3±0.9 | 5.2±0.9 | < .05 |
| SBP, mmHg | 128.3±21.6 | 134.0±19.1 | 123.3±22.5 | < .001 |
| DBP, mmHg | 77.4±10.9 | 79.7±10.0 | 75.3±11.2 | < .001 |
| BMI | 28.8±5.1 | 29.2±4.4 | 28.5±5.7 | < .01 |
| Waist circumference, cm | 98.3±13.0 | 100.6±11.1 | 96.2±14.1 | < .001 |
| Smokers | 690 (31.2) | 397 (38.1) | 293 (25.0) | < .001 |
| Obesity | 806 (36.4) | 394 (37.8) | 412 (35.2) | .205 |
| Abdominal obesity | 1252 (56.6) | 437 (41.9) | 815 (69.7) | < .001 |
| Hypercholesterolemia | 783 (35.4) | 377 (36.2) | 406 (34.7) | .468 |
| Drug-treated hypercholesterolemia | 380 (48.5) | 177 (46.9) | 203 (50.0) | < .05 |
| Lipid-lowering drugs | 380 (17.2) | 177 (17.0) | 203 (17.4) | .821 |
| Hypertension | 894 (40.4) | 465 (44.6) | 429 (36.7) | < .001 |
| Diabetes mellitus | 305 (13.8) | 161 (15.5) | 144 (12.3) | < .05 |
| Metabolic syndrome | 789 (35.7) | 345 (33.1) | 444 (37.9) | < .05 |
| CKD | 100 (4.5) | 33 (3.2) | 67 (5.7) | < .01 |
| Peripheral artery disease | 119 (5.4) | 66 (6.3) | 53 (4.5) | .060 |
| Cerebrovascular disease | 28 (1.3) | 19 (1.8) | 9 (0.8) | < .05 |
| Ischemic heart disease | 48 (2.2) | 28 (2.7) | 20 (1.7) | .114 |
| Ischemic heart disease, cerebrovascular disease or revascularization | 79 (2.9) | 47 (3.8) | 32 (2.2) | < .05 |
ApoA, apolipoprotein A; ApoB, apolipoprotein B; BMI, body mass index; CKD, chronic kidney disease; DBP, dystolic blood pressure; HDL-C, high-density lipoprotein cholesterol; LDL-C low-density lipoprotein cholesterol; SBP, systolic blood pressure.
Data are expressed as mean±standard deviation, No. (%), or median [interquartile range].
Analysis of CVR distribution showed that 27.1% of men were in the very high or high risk categories compared with 20.8% of women (P<.05). In contrast, 75.6% of women were at low CVR compared with 56.8% of men (P<.001). Of participants at very high or high CVR, 51.9% of men were taking lipid-lowering drugs vs 33.7% of women (P<.05); in the low CVR category, 8.8% of men were taking lipid-lowering drugs vs 12.7% of women (P<.05). Our study did not investigate the dose or type of drug prescribed, but given the prescription pattern of lipid-lowering drugs in the health system, it can be assumed that most were statins.
The degree of attainment of target LDL-C levels in each CVR category is shown in Table 2. The data reveal that only 6.5% of the population at very high or high risk achieved target LDL-C levels, most of them men (8.9% vs 3.7%; P<.01). However, in the low and moderate CVR categories, a higher percentage of women achieved target LDL-C levels (Table 2). In the multivariable analysis, only female sex was associated with worse lipid control in the very high and high risk groups (odds ratio [OR]=2.25; 95% confidence interval [95%CI], 1.01-5.00; P<.05), whereas a history of cardiovascular disease was associated with better lipid control (OR=0.23; 95%CI, 0.11-0.52; P<.001).
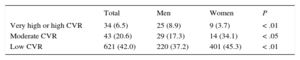
Population Achieving Target Levels of Low-density Lipoprotein Cholesterol Stratified According to Cardiovascular Risk Category
| Total | Men | Women | P | |
|---|---|---|---|---|
| Very high or high CVR | 34 (6.5) | 25 (8.9) | 9 (3.7) | < .01 |
| Moderate CVR | 43 (20.6) | 29 (17.3) | 14 (34.1) | < .05 |
| Low CVR | 621 (42.0) | 220 (37.2) | 401 (45.3) | < .01 |
CVR, cardiovascular risk.
Target levels of low-density lipoprotein cholesterol: < 70mg/dL for patients at very high CVR, < 100mg/dL for patients at high CVR, and < 115mg/dL for patients at moderate or low CVR. Data are No. (%).
Finally, for patients with diseases requiring secondary prevention goals, the highest percentage of target LDL-C was achieved among those with cardiovascular disease (ischemic heart disease and stroke; 17.7% of patients had LDL-C<70mg/dL; 23.4% of men vs 9.4% of women; P=.140). The second highest percentage was achieved among those with peripheral artery disease (LDL-C<70mg/dL, 9.2%; 15.2% in men, 1.9% in women; P<.05).
In summary, our study reveals that 48.9% of patients with very high or high CVR are prescribed lipid-lowering drugs, but that the prescription rate among women in these risk categories is lower than for men (33.7% vs 51.9%; P<.05); moreover, among patients in these risk categories, a lower proportion of women than men achieve target LDL-C levels (3.7% vs 8.9%; P<.05). In contrast, a higher proportion of women than men at moderate or low CVR take lipid-lowering drugs (34.7% vs 22.4%; P<.05) and a higher proportion of them have target LDL-C levels (79.4% vs 54.5%; P<.05) (Table 2).
These results are consistent with those of other studies indicating that different therapeutic approaches to CVR are used for women and men: there is a tendency to undertreat women in secondary prevention and those at very high or high CVR, and a tendency to overtreat women at moderate of low CVR. The evidence thus indicates that women at very high or high CVR receive less effective treatment than men in the same risk categories.
Our study highlights the value of research into strategies aimed at increasing health care professionals’ awareness of the need for gender equality in the approach to CVR, especially in relation to women in secondary prevention or at very high or high risk. This would also result in a more efficient use of lipid-lowering drugs.
FUNDINGPlan Nacional de Investigación Científica 2004-2007 (PI071218), Río Hortega (CM08/00141) contract from the Instituto de Salud Carlos III, Fellowship from the Plan Integral de Enfermedades Cardiovasculares de Extremadura, Fundesalud, Junta de Extremadura.