Although the incidence of Listeria monocytogenes infections is increasing,1 infective endocarditis (IE) is still an uncommon and poorly studied disease, with only case reports and reviews reported in the literature.2,3
Listeria is a nonsporulating, aerobic, Gram-positive coccobacillus. Listeria. monocytogenes is only considered pathogenic in humans, behaving as a zoonosis. It is usually acquired from food and causes disease as an opportunistic infection in newborns, pregnant women, and immunocompromised patients, although it can also affect healthy individuals. Its clinical presentation is diverse; miscarriage, sepsis, and meningoencephalitis are common, and it is generally associated with high morbidity and mortality.2
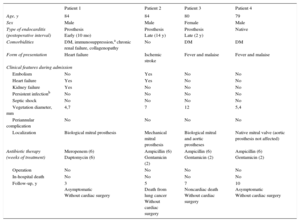
The aim of this work was to describe the characteristics of patients with IE caused by L. monocytogenes who were treated in 3 Spanish hospitals considered referral centers for this disease. From a multipurpose database containing 1374 IE episodes consecutively diagnosed between January 1995 and November 2015, we selected those caused by L. monocytogenes. The characteristics of the 4 patients (0.3%) identified are described in the Table.
Summary of the Characteristics of the Patients With Listeria monocytogenes
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | |
|---|---|---|---|---|
| Age, y | 84 | 84 | 80 | 79 |
| Sex | Male | Male | Female | Male |
| Type of endocarditis (postoperative interval) | Prosthesis Early (10 mo) | Prosthesis Late (14 y) | Prosthesis Late (2 y) | Native |
| Comorbidities | DM, immunosuppression,a chronic renal failure, collagenopathy | No | DM | DM |
| Form of presentation | Heart failure | Ischemic stroke | Fever and malaise | Fever and malaise |
| Clinical features during admission | ||||
| Embolism | No | Yes | No | No |
| Heart failure | Yes | Yes | No | No |
| Kidney failure | Yes | No | No | No |
| Persistent infectionb | No | No | No | No |
| Septic shock | No | No | No | No |
| Vegetation diameter, mm | 4,7 | 7 | 12 | 5,4 |
| Periannular complication | No | No | No | No |
| Localization | Biological mitral prosthesis | Mechanical mitral prosthesis | Biological mitral and aortic prostheses | Native mitral valve (aortic prosthesis not affected) |
| Antibiotic therapy (weeks of treatment) | Meropenem (6) Daptomycin (6) | Ampicillin (6) Gentamicin (2) | Ampicillin (6) Gentamicin (2) | Ampicillin (6) Gentamicin (2) |
| Operation | No | No | No | No |
| In-hospital death | No | No | No | No |
| Follow-up, y | 3 Asymptomatic Without cardiac surgery | 5 Death from lung cancer Without cardiac surgery | 7 Noncardiac death Without cardiac surgery | 10 Asymptomatic Without cardiac surgery |
DM, diabetes mellitus.
Although we cannot draw any conclusions because of the small number of patients, our patients do show some common features. The patients were all elderly, older than previously reported ages for infections of this bacteria.1,2 Although L. monocytogenes typically affects women, IE is more frequent in men, particularly in the setting of prosthetic endocarditis.2 Three of the 4 patients in our series were diabetic, and all had received a valve prosthesis, although the IE exclusively affected a native valve in 1 of the patients. Both factors (diabetes mellitus and prosthesis) have been associated with IE due to L. monocytogenes,2 probably because of the tendency of this bacterium to affect immunocompromised patients and those with predisposing factors. All of our patients showed mitral valve involvement, the most commonly affected site in prosthetic disease (52%).2 Regarding the mechanism of transmission, there is little information in the literature on the history of the consumption of possibly contaminated food, and we were also unable to verify this datum in our patients.
The most frequent focus of L. monocytogenes infection is the central nervous system.1 In the case of IE, various forms of presentation have been described in the literature, from localized infections to systemic symptoms with a fulminant course.3 Our 4 patients showed diverse forms of presentation, with a relatively benign clinical course. Notably, despite the evidence of IE,4 all 4 patients received medical treatment, without increased in-hospital mortality or long-term follow-up. Although L. monocytogenes infections are associated with elevated mortality,1 particularly in the setting of IE,2 lower mortality has been described in patients with prosthetic endocarditis than in those with native valve endocarditis.2 The antibiotic therapy recommended for Listeria infections is based on a combination of ampicillin and gentamicin. The evidence for this approach is weak: there are no comparative studies, only the results of large series5 and a theoretical synergistic effect in in vitro studies.6 This antibiotic regimen was used in our patients, except in patient 1, who was allergic to penicillin and had chronic renal failure. This patient was thus treated with combination meropenem and daptomycin in accordance with the antimicrobial susceptibility profile.
In conclusion, IE due to L. monocytogenes is an uncommon condition tending to affect elderly patients and those with diabetes and prosthetic valves. Antibiotic therapy with ampicillin and gentamicin is a suitable therapeutic option, at least in patients with a good clinical course.