
High-definition intravascular ultrasound (HD-IVUS) that uses 60MHz transducers is the latest advance in the development of this imaging technique. HD-IVUS allows not only higher spatial resolution, but also faster acquisition speed (withdrawal speed of up to 10mm/s, at 60 images/s) than conventional 40MHz IVUS.1–3 However, currently there is little evidence to advocate its clinical use.1 The aim of the present study was to prospectively analyze the usefulness of HD-IVUS in a small series of consecutive patients, by comparing the findings with those obtained from optical coherence tomography (OCT).
We selected 4 consecutive patients who, after providing signed, informed consent, were systematically examined with HD-IVUS and OCT in the proximal and medial segments of 2 coronary arteries (8 arteries in total). One of the 4 patients underwent percutaneous coronary intervention with stent implantation, after which both imaging techniques were repeated. For the HD-IVUS study, we used a Kodama catheter (ACIST Medical Systems; Eden Prairie, Minnesota, USA) at 10 mm/s, and for OCT, we used a Dragonfly OPTIS catheter (St Jude Medical; St Paul, Minnesota, USA) with an angiographic coregistration system. For quantitative analysis, we selected different 5 mm-long segments of coronary artery and looked at the potentially relevant OCT findings in each artery studied (presence of atherosclerotic plaque, stented segment) or postintervention findings. As a reference, we used different markers (branches, stent edge) to ensure that exactly the same coronary segments were analyzed with both techniques. In these segments, we determined, frame by frame, both the luminal area (LA) and the atheroma characteristics with both techniques. In stented segments, we assessed strut endothelialization, possible stent malapposition or underexpansion, and the occurrence of dissections after implantation. Quantitative data were compared using the Bland-Altman method. The mean age was 67 ± 12 years and 3 of the 4 patients were male. In 3 patients, the indication for coronary angiography was angina with a positive stress test, whereas the fourth patient underwent a scheduled follow-up angiography 9 months after revascularization. In 3 patients, we evaluated the left anterior descending and right coronary arteries, and in the fourth patient, the left anterior descending and the circumflex arteries. Figure 1 shows some of the images acquired with both techniques at the same position. In general, both techniques allowed us to correctly evaluate the presence of normal segments, detect atherosclerotic plaques and determine their characteristics, and detect the presence of calcium. Due to its higher resolution, OCT proved superior to HS-IVUS for identification of small intimal flaps after intervention, as well as in the evaluation of the degree of strut endothelialization and the presence of evaginations in the stent at follow-up. However, in all patients, both techniques allowed us to correctly identify stent malapposition and underexpansion. For quantitative analysis, a total of 400 frames of the selected segments were analyzed with both techniques. Figure 2A illustrates, with a Bland-Altman plot, the excellent concordance for LA determination. Figure 2B shows (for illustrative purposes) the data on the linear relationship between the 2 techniques for LA determination, evaluated quantitatively with determination of the intraclass correlation coefficient.
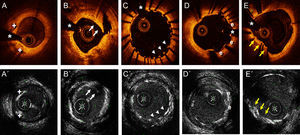
. B and B’ show the immediate result after semicompliant balloon predilatation of a severely calcified lesion in the circumflex artery, with an image of an intimal flap (arrows) compatible with dissection. C and C’ show the result at 9 months post implantation of a drug-eluting stent in the proximal right coronary artery, demonstrating the absence of strut endothelialization in 2 thirds of the circumference, as well as an area of malapposition (arrowheads). D and D’ show the development of evaginations (e) in a drug-eluting stent implanted 9 months earlier. E and E’ show an area of underexpansion in a drug-eluting stent implanted 9 months earlier, due to the presence of a highly-calcified eccentric plaque (arrows). *Artefact from guidewire.")
The upper row of images shows the findings from optical coherence tomography, and the lower row of images shows the findings from high-definition intravascular ultrasound. A and A’ show an area of fibrocalcified plaque in the left anterior descending artery, where 2 calcified nodules are demarcated (+). B and B’ show the immediate result after semicompliant balloon predilatation of a severely calcified lesion in the circumflex artery, with an image of an intimal flap (arrows) compatible with dissection. C and C’ show the result at 9 months post implantation of a drug-eluting stent in the proximal right coronary artery, demonstrating the absence of strut endothelialization in 2 thirds of the circumference, as well as an area of malapposition (arrowheads). D and D’ show the development of evaginations (e) in a drug-eluting stent implanted 9 months earlier. E and E’ show an area of underexpansion in a drug-eluting stent implanted 9 months earlier, due to the presence of a highly-calcified eccentric plaque (arrows). *Artefact from guidewire.
 the close linear relationship between the 2 techniques for luminal area determination, determined quantitatively from the ICC. HD-IVUS, high-definition intravascular ultrasound; ICC, intraclass correlation coefficient; OCT, optical coherence tomography.")
A: Bland-Altman plot showing the excellent concordance between HD-IVUS and OCT for luminal area determination. B: (illustrative only) the close linear relationship between the 2 techniques for luminal area determination, determined quantitatively from the ICC. HD-IVUS, high-definition intravascular ultrasound; ICC, intraclass correlation coefficient; OCT, optical coherence tomography.
Until now, only isolated cases have been published of coronary images obtained with HD-IVUS.1 The present study is the first small series to evaluate this new technology. HD-IVUS achieves a far superior image quality with an acquisition time 10 times faster than conventional IVUS. Unlike previous studies that demonstrated that conventional IVUS tended to overestimate LA compared with OCT,4 in our study this phenomenon did not occur with HD-IVUS, and there was excellent concordance for LA measurement between HD-IVUS and OCT; however, due to the lower spatial resolution, HD-IVUS was inferior for evaluating adequate device endothelialization. However, by avoiding some of the classic limitations of OCT (aorto-ostial lesions, shadows from thrombotic material, need for contrast) and improving the resolution of conventional IVUS, HD-IVUS may represent a new tool of great interest in both clinical practice and research.