To the Editor,
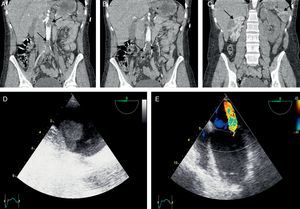
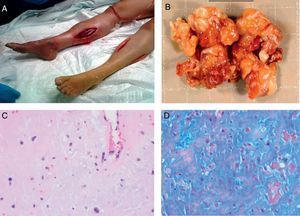
A 37-year-old woman with no relevant history came to the emergency room reporting dizziness, acute abdominal pain, and weakness as well as pain and dysesthesia in the lower limbs. The physical examination revealed sinus tachycardia, sweating, altered mental state, and hypotension. A cranial computed tomography (CT) scan and substance abuse screening of the urine showed no abnormalities. The examination of the lower limbs showed no right femoral pulse, a weak left femoral pulse, and signs of poor skin perfusion in both limbs. The chest and abdominal CT scans revealed severe occlusion of the infrarenal aorta (Figure 1A), acute occlusion of the 2 common iliac arteries, left renal artery thrombosis showing images consistent with infarction of the ipsilateral kidney (Figure 1B), and segmental infarctions in the spleen and the right kidney (Figure 1C). Intravenous heparin sodium was started, the patient was intubated and connected to mechanical ventilation, and vasoactive drug therapy was initiated to treat the shock. Transthoracic echocardiography showed left ventricular dilatation with an ejection fraction of 15%, severe mitral regurgitation due to restriction of the posterior leaflet, and a mass in the left atrium (1.9×2.2 cm). The transesophageal echocardiographic study (Figure 1D and E) confirmed the presence of a hypermobile mass with multiple finger-link projections; the mass was adhered to the interatrial septum and highly consistent with cardiac myxoma. The patient underwent proximal and distal percutaneous embolectomy with bilateral femoral access as well as multiple compartment fasciotomy of both limbs (Figure 2A). The intravascular material fragments removed (Figure 2B) were sent for histologic study, which confirmed cardiac myxoma embolism (Figure 2C and D). The patient experienced hyperpotassemia (7.1 mEq/L) and an increase in creatine kinase concentration (121 500 IU/L) secondary to the reperfusion lesion, which required venovenous hemofiltration. The patient died a few hours later due to multiorgan failure.

Figure 1. A, chest and abdominal computed tomography scan; infrarenal aortic occlusion and left renal artery thrombosis. B, chest and abdominal computed tomography scan; bilateral occlusion of the common iliac arteries. C, chest and abdominal computed tomography scan; segmental infarctions of the spleen and the right kidney. D, transesophageal echocardiography; finger-like cardiac mass in the left atrium. E, transesophageal echocardiography; mitral regurgitation caused by restriction of the posterior leaflet of the mitral valve.

Figure 2. A, fasciotomy of both legs with clear signs of hypoperfusion. B, fragments of removed intravascular material (scale bar, 20 mm). C and D, microphotographs (hematoxylin and eosin, ×100; PAS- Alcian blue, ×400) showing the characteristic histology of myxoma fragments.
Primary tumors of the heart are rare, with an estimated incidence between 0.0017% and 1.9% of unselected patients in autopsy studies. Among malignant tumors, sarcoma is the most common type, followed by angiosarcoma.1 Atrial myxoma is the most common benign tumor of the heart (approximately 50% of primary cardiac tumors). These tumors occur slightly more often in women, and usually present in patients aged 30 to 60 years. Although histologically benign, they are occasionally fatal due to their strategic intracardial position. Three-fourths of all myxomas are found in the left atrium.2 The tumors are often underdiagnosed due to the lack of specific symptoms. The clinical manifestations can include congestive heart failure, hemoptysis, cough, transient cyanosis, syncope, dyspnea, neurologic symptoms or pain in ischemic limbs due to cardiac obstruction (as a result of tumor fragmentation or, less often, complete tumor rupture), or arrhythmias. Atrial myxomas are a rare cause of acute peripheral arterial ischemia.3 Ventricular dysfunction occasionally occurs and can be caused by myocardial infarction due to tumor fragment embolism in the coronary arteries or an acute increase in peripheral resistances resulting from complete acute occlusion of the infrarenal aorta (in our patient, both mechanisms were possible). In conclusion, in young, healthy patients, cardiac myxoma should be considered in the differential diagnosis of peripheral arterial embolism.
.
Corresponding author: maapalomares@secardiologia.es