

Cardiac magnetic resonance, and particularly the more recently developed sequences of parametric mapping, play an important role in the differential diagnosis of ventricular hypertrophy. This usefulness is highlighted in the recently published case by Oliveira et al.,1 in which they present a patient with severe myocardial hypertrophy and inferolateral late enhancement, a typical, though not specific, area for cardiac involvement in Fabry disease. The finding of reduced native T1 values in the septum strongly indicated the diagnosis, which was confirmed with laboratory tests and genetic study.
Beyond the clinical situations such as the above, T1 mapping is useful in another aspect of Fabry disease, that we believe should be highlighted: the early detection of cardiac involvement. This is of particular interest in patients who are carriers of a pathogenic variant who have not developed a clear phenotype.
By way of example of this clinical use, we present the case of a 30-year-old man who attended the familial heart disease clinic for screening for Fabry disease. He was from a large family of carriers of the pathogenic variant p.Arg301Gln of the gene for galactosidase A. Both his 63-year-old mother and his 39-year-old brother were on treatment for renal and cardiac disease (figure 1, family tree). He was a healthy, sporty individual, with no findings of note on history or targeted physical examination. Baseline electrocardiogram and echocardiogram were normal (ruled out ventricular hypertrophy).

Genetic study revealed that the patient was a heterozygotic carrier of the familial variant p.Arg301Gln. Blood tests showed a reduced activity of alpha-galactosidase and an increase in serum concentrations of globotriaosylsphingosine (lyso-Gb3, 4.79ng/mL; normal, < 1.4ng/mL). Renal function was normal, although with 24-hour urine microalbumin levels toward the upper limit of normal (29.8mg/24 h; normal, 0-30mg/24 h).
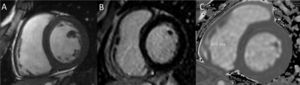
The phenotype study was continued with cardiac magnetic resonance that showed morphological findings in line with the echocardiogram, with no ventricular hypertrophy (interventricular septum of 9mm) and preserved biventricular function (figure 2A). Late enhancement study was negative (figure 2B). On the T1 mapping sequence the native T1 value was 805ms, lower than the local reference values (904-1040ms) and compatible with incipient heart involvement from Fabry disease (figure 2C).

In summary, this was a young man who was a carrier of the pathogenic variant p.Arg301Gln for Fabry disease, with raised plasma LysoGb3 levels, findings of incipient cardiac involvement (reduced native T1) and possible renal involvement (microalbuminuria at the upper limit of normal). Furthermore, he was from a family with a phenotype of early clinical presentation. Considering all of this information, it was decided to offer specific treatment, and the patient was started on migalastat.
Parametric mapping sequences improve the capacity of cardiac magnetic resonance to characterize the myocardium and allow the detection of insipient or diffuse tissue abnormalities, without the administration of contrast.
In Fabry disease, there is an intracellular accumulation of glycosphingolipids that lead to hypertrophy and finally apoptosis and fibrosis. In the early phases, even without observable hypertrophy, mapping sequences show a reduced native T1 associated with the lipid accumulation.2 In the intermediate phases, there is ventricular hypertrophy, and in the more advanced phases, fibrosis, identified on the basis of pseudonormalized or increased native T1 values, as well as late gadolinium enhancement in the affected area, typically the inferolateral segments. In this phase, an increase in T2 values has also been described, probably in relation to a degree of chronic inflammation.3,4
Therefore, in addition to the differential diagnosis in cases of hypertrophy, parametric mapping sequences can be useful in the early diagnosis of cardiac involvement in Fabry disease, as this is the earliest known imaging parameter affected. This, together with the rest of the clinical and laboratory parameters, the characteristics of the genetic variant, and the family history, allows identification of patients in the early phase who may benefit from a closer follow-up or potential specific treatment in cases such as the one presented here.4
No written informed consent was obtained for the publication of this case, as no images or identifying patient data are presented.
FUNDINGNone.
AUTHORS’ CONTRIBUTIONSV. Ruiz Pizarro wrote the first draft of the manuscript and created the figures. J. Álvarez Rubio, T. Ripoll-Vera, and M.J. Soleto Roncero provided comments on subsequent modifications and reviewed the final version.
CONFLICTS OF INTERESTJ. Álvarez Rubio declares having received fees for presentations from Amicus Therapeutics and Shire. The rest of the authors have no conflicts of interest regarding this article.