Keywords
INTRODUCTION
A heart with a criss-cross atrioventricular (AV) connection is a cardiopathy in which the ventricles are positioned contralaterally to the atria to which they are connected; the ventricular inflow tracts are crossed, hence the name criss-cross.
In 1961 various cases of AV discordance with or without ventriculoarterial (VA) discordance were described. One of those cases presented as situs solitus with dextrorotation of the cardiac loop, which could correspond to the description of this abnormality.1 In 1973, for the first time, in Mexico a report was published of a 4-month-old boy with situs solitus with AV concordance, VA discordance, and crossing of the ventricular inflow chambers, with anterosuperior right ventricle (RV) and posterior and inferior left ventricle (LV), ventricular septal defect (VSD), and pulmonary stenosis (PS).2 These cases were later given the name of criss-cross.3
In the later years, other cases were described: 37 with situs solitus, 2 with situs inversus, and 1 with isomerism, most with AV concordance.4,5
The most common VA connection was discordant transposition of the great arteries (TGA), followed by double outlet RV (DORV), associated with PS and even more rarely with pulmonary atresia.4-6
The most common is atrial situs solitus presentation with right atrium (RA) connected to left-sided RV with anterior tricuspid valve and left aorta, as well as left atrium (LA) connected to right-sided LV with mitral valve oriented in the posterior direction. Criss-cross heart is often associated with superior-inferior ventricles; this ventricular relationship can present in other cardiopathies.7
In many cases, the size of the ventricles (small on many occasions) is conditioned by the size of the annulus of the AV valves.8,9
The physiology is determined by the discordant or concordant AV and VA connection and the associated cardiac defects, such as displaced and/ or straddling left AV valve, VSD (which always presents), valvular or subvalvular PS, small RV, and juxtaposition of the atrial appendages.7,10-12
Another of its hemodynamic characteristics is that the systemic and pulmonary venous systems are crossed at the AV level, although without mixing.
Two-dimensional echocardiography, with subcostal and 4-chamber views, can be used to identify the ventricular morphology and position, the AV valves, the AV and VA connection, and the characteristics of the great vessels. The artery connection can be seen more clearly in the parasternal window.13
METHODS
Over a 5-year period, 8567 studies were performed in our echocardiography laboratory; criss-cross heart was diagnosed in 5 patients.
A retrospective, observational, longitudinal study was carried out, analyzing age, gender, and symptoms. The echocardiographic study was based on the segmental sequential approach used to diagnose congenital heart diseases.14 The study identified the situs, AV and VA connection, spatial position of the ventricles and interventricular septum, characteristics of the arterial vessels, ventricular size, other associated cardiac lesions, and the orientation of the aortic arch. Because the level of implantation of the AV valves is difficult to define in this condition, ventricular morphology was defined by the characteristics of the subvalvular apparatus, RV moderator band and trabeculations. Blood flow characteristics and directions were analyzed by color Doppler ultrasound. In 3 patients, the echocardiographic findings were compared to the cardiac catheterization study to confirm the diagnosis.
All studies were carried out with Hewlett-Packard Agilent 5500 echocardiography system using 3-MHz and 8-MHz transducers.
Patients with hearts in which the superior-inferior ventricles did not present criss-cross were excluded from the study.
RESULTS
Criss-cross heart was diagnosed in 5 (0.06%) of the 8567 studies. Patient age ranged between 1 month and 20 years (mean, 6 years and 3 months); 4 were female and 1 was male. The predominant clinical signs were systolic murmur in the aortic area in all patients, manifestations of heart failure in 4, and cyanosis in 3.
All 5 patients presented situs solitus and levocardia on echocardiographic segmental analysis. Pulmonary venous return was normal in all patients, and none had juxtaposition of the atrial appendages.
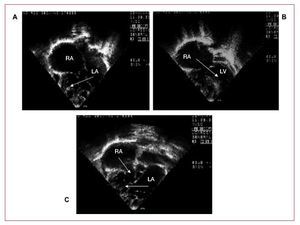
The AV connections were discordant in 3 cases and concordant in 2. The tricuspid valve showed regurgitation in 2 patients (1 with valve dysplasia) and was normal in 3. Hypoplastic mitral valve was present in 1 patient and straddling mitral valve in 2. The interventricular septum was vertical in 3 patients and horizontal in 2, with superior-inferior ventricles. In 3 patients, the LV was small (Figures 1 and 2). Regarding the VA connection, 4 patients presented DORV and 1, concordance with imperforate pulmonary valve (IPV).

Figure 1. Two-dimensional echocardiography of Patient 3 in 4-chamber apical view. A, left atrium (LA) connected to a right-sided morphologic right ventricle (RV) with atrioventricular discordance and straddling mitral valve. B, right atrium (RA) connected to a left-sided morphologic left ventricle (LV). C, atrioventricular crossover with vertically oriented ventricles.

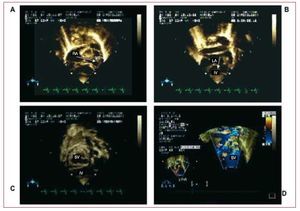
Figure 2. Two-dimensional color echocardiography of Patient 5, in subcostal view. A: right atrium (RA) connected to a superior ventricle (SV). B: left atrium (LA) connected to an inferior ventricle (IV), with atrioventricular concordance. C: superior ventricle (SV) and inferior ventricle (IV). D: double-outlet superior ventricle (SV) with right-sided aorta (Ao) and left-sided pulmonary artery (PA).
The associated cardiac lesions were large VSD in all patients (1 perimembranous; 2 subaortic, 2 inflow tract); 1 had multiple VSDs. In 3 patients, mixed-type PS was present; persistent ductus arteriosus in 3, and atrial septal defect in 3; 1 patient had hypoplastic aortic arch. The aortic arch was left-sided in 4 cases and right-sided in 1 (Table 1).

A hemodynamic study was performed in 3 patients and was consistent with the echocardiographic diagnoses.
To our knowledge, none of the 5 patients died during clinical follow-up.
DISCUSSION
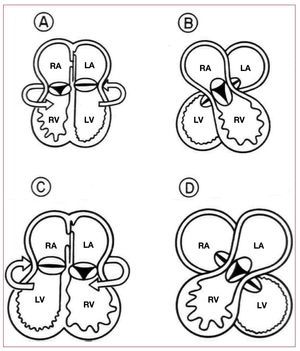
Criss-cross heart is a rare, complex congenital heart malformation. The ventricles twist around their long axis, with no concomitant movement of the atria, thus producing crossing of the inflow tracts. In a crossed AV connection, the ventricles are contralateral to the atria to which they are connected. This abnormal position is explained by twisting of the ventricular mass (once the AV connection has been established). When twisting over the ventricular long axis is counterclockwise in concordant AV connections, the right-sided RA remains connected to the right ventricle (RV) spatially located in the anterior and left position; this leads to a discordant AV relationship (Figure 3A and B). When the AV connections are discordant, the twist is clockwise and the left-sided LA is connected to the RV, located in the anterior and right position, which determines a concordant AV relationship15-17 (Figure 3C and D).

Figure 3. Anterior view (from the observer). Diagram of the cardiac chambers illustrating the etiologic mechanism (ventricular twist) that causes criss-cross heart. A: atrioventricular (AV) concordance; ventricular twist is counterclockwise. B: AV concordance with discordant spatial relationship: right-sided morphologic right atrium (RA) connected to a left-sided morphologic right ventricle (RV) and left-sided morphologic left atrium (LA) connected to a right-sided morphologic left ventricle (LV). C: AV discordance; ventricular twist is clockwise. D: AV discordance with concordant spatial relationship: right-sided morphologic RA connected to a left-sided morphologic LV and left-sided morphologic LA connected to a right-sided morphologic RV.
This disorder can be interpreted as the crossing of systemic and pulmonary venous blood without mixing in the AV valves.3
In the criss-cross heart, the ventricles are often related top to bottom (superior-inferior), displacing the ventricular mass in the horizontal plane. However, this is not an essential condition. In our study, only 2 of the 5 patients presented superior-inferior ventricles.
The VA connection should be described separately from the relationship of the chambers and arteries with the AV connection.17 The VA connection is extremely variable: discordant is the most common type reported in the literature, followed by DORV. The VA relationship may be concordant or discordant, and PA rarely presents.18 In our study, DORV was most common and 1 patient had IPV (Table). Abnormalities in the coronary arteries, such as underdeveloped or absent left anterior interventricular artery, have also been reported.19
Up to 1999, 97 cases of patients with criss-cross heart had been published, of which only 14 presented double discordance.20
A complete anatomic and physiologic diagnosis can be established in this condition using 2-dimensional echocardiography, along with other diagnostic methods such as magnetic resonance imaging, if necessary.21,22
The type of connection (AV or VA) and characteristics of associated lesions (VSD, PS, straddling mitral valve, and small ventricles) determine the clinical and hemodynamic manifestations in patients with criss-cross heart and can be used to guide the surgical repair.16
One of the difficulties for the surgeon is to locate the branch of the His bundle in VSD repair. Biventricular surgical repair is the option in some criss-cross cases. In patients who also present DORV or TGA and have ventricles of adequate size, the repair should be accompanied by a patch on the ventricular septal defect and an atrial or arterial switch. If PS is present, a systemic-pulmonary shunt must be performed; however, RV size and tricuspid valve displacement may be limitations for good surgical outcome.9,23 In patients who cannot undergo biventricular surgical repair, palliative surgery with the modified Glenn and Fontan technique for definitive repair is proposed.13
The condition can be more clearly understood if the defects are observed separately because crisscross hearts are characterized by concomitant multiple lesions and rarely present alone.19
In conclusion, patients with criss-cross heart can be diagnosed by a careful, systematic segmental study with 2-dimensional color-coded transthoracic echocardiography to determine the sequence of connections and spatial relationships of the cardiac chambers and identify other abnormalities.
Correspondence: Dr. J. de Rubens Figueroa.
Juan Badiano, 1, Col. Sección XVIII. Delegación Tlalpan. CP 14080. México DF. México.
E-mail: derubens@hotmail.com
Received December 12, 2007.
Accepted for publication December 16, 2008.