
Pulmonary arterial hypertension (PAH) affects almost 4% of patients with congenital heart disease (CHD),1 worsening their prognosis. After pulmonary vasodilator therapy, the only remaining therapeutic option is double lung transplant, frequently accompanied by heart transplant. Nevertheless, access to heart-lung transplant is increasingly limited by the scarcity of donor organs and the high risk involved.
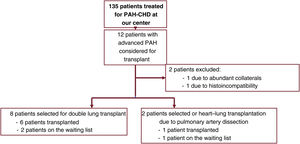
In the present study, we retrospectively analyzed the case histories of patients with PAH-CHD who underwent double lung transplant at our center from September 2010 to January 2022. This is the first such patient series described in Spain. The indication for transplant was high-risk PAH despite optimized medical treatment with triple vasodilator therapy including intravenous prostacyclins. During the study period, 12 of the 135 PAH-CHD patients treated at our center were considered for transplant (figure 1). Of these 12 patients, 6 underwent double lung transplant, representing 13% of patients undergoing this procedure for PAH at our center during the study period. The patients gave informed consent for the intervention and for the publication of the study findings. The mean age of the patients was 39±10, and 67% were women. All the patients had a history of heart failure. Of the 6 patients, 4 had typical atrial flutter and were treated by ablation of the cavotricuspid isthmus; arrhythmia recurrence was recorded in 2 of these patients, 1 with atypical incisional atrial flutter and another with atrial fibrillation. Pulmonary artery trunk aneurysm with a maximum diameter of 53mm was found in 4 patients; in 1 patient the aneurysm was complicated by symptomatic extrinsic compression of the left coronary artery, requiring implantation of an intracoronary stent, and another patient had in situ thrombosis in the pulmonary artery trunk. Finally, 1 patient had life-threatening hemoptisis requiring bronchial artery embolization. Regarding etiology, 2 patients had residual PAH years after closure of the intracardiac defect, and the remaining 4 had an incidental intracardiac shunt. Due to suspicion of pleural adhesions in the 2 patients with residual PAH after previous defect repair, extracorporeal circulation was established with femoral cannulation. In the 4 patients with open defects, central cannulation was used, and the defects were closed during the transplant procedure, with the exception of a restrictive interventricular communication that was left open. Defect closure did not significantly increase the duration of extracorporeal circulation (284minutes without closure vs 299minutes with closure). The presence of pulmonary aneurysm increased the complexity of arterial anastomosis, whereas no modification of the procedure was required in the patient with in situ thrombosis. There were 2 severe postsurgery complications: 1 patient developed interstitial pulmonary edema, prolonging intubation and requiring hemofiltration; and another patient had bleeding with hemodynamic consequences related to the clamshell incision and required reintervention. These are both frequent complications of double lung transplant for PAH, but neither occurred in the patients with previous sternotomy. Median time in the intensive care unit was 10 [interquartile range, 9-12] days. All patients were discharged and were alive at the time of writing, with the first patient surviving more than 11 years to date. Remarkably, none of the patients has had subsequent cardiovascular complications or arrhythmias. Moreover, at the 6-month follow-up, all the patients showed appropriate positive right ventricular remodeling, with size normalization and full functional recovery (table 1).

Baseline characteristics and echocardiographic changes in PAH-CHD patients undergoing double lung transplant.
| Age at Tx | Sex | Time since Tx, y | PAH-CHD type | Previous HF | Previous arrhythmias | RA diameter at rest pre-Tx, mm | RA diameter at rest post -x, mm | RA dysfunction pre-Tx | RA dysfunction post-Tx | TAPSE pre-Tx, mm | TAPSE post-Tx, mm | RA pre-Tx, cm2 | RA post-Tx, cm2 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 23 | M | 11 | Incidental IVC | Yes | No | 51 | 35 | Moderate | No | 13 | 17 | 28 | 17 |
| 36 | W | 9 | Incidental IAC | Yes | ICT flutter | 43 | 38 | Severe | No | 14 | 17 | 27 | 14 |
| 37 | W | 7 | Incidental IAC | Yes | No | 54 | 30 | Severe | No | 13 | 18 | 24 | 13 |
| 48 | W | 3 | Incidental IVC | Yes | Flutter | 43 | 35 | Moderate | No | 13 | 18 | 29 | 14 |
| 51 | W | 1 | IAC after defect closure | Yes | CTI and incisional flutter | 60 | 39 | Severe | No | 15 | 17 | 29 | 20 |
| 44 | M | 1 | IVC after defect closure | Yes | CTI flutter Paroxysmal AF | 52 | 38 | Moderate | No | 17 | 18 | 33 | 22 |
| Median [interquartile range] | 5 [1-9] | Mean | 51±7 | 36±3 | 14±2 | 18±1 | 28±3 | 17±4 | |||||
| P=.02 | P=.02 | P < .01 | |||||||||||
AF, atrial fibrillation; CHD, congenital heart disease; CTI, cavotricuspid isthmus; HF, heart failure; IAC, interatrial communication; IVC, interventricular communication; M, man; PAH, pulmonary arterial hypertension; RA, right atrium; RV, right ventricle; TAPSE, tricuspid annular plane systolic excursion; Tx, transplant; W, woman.
PAH normally progresses to right ventricular failure and heart failure despite vasodilator therapy, leaving transplant as the only option. The choice of transplant technique remains a subject of debate. Some comparisons of lung and heart-lung transplant in PAH patients have reported similar outcomes, reflecting the rapid right ventricular recovery after isolated lung transplant.2 However, many centers still regard cardiac defects and the frequent presence of pulmonary artery aneurysms3 as indications for heart-lung transplant. Due to the scarcity of donor hearts and the risk of the heart-lung transplant procedure, double lung transplant with concomitant surgical repair of simple cardiac defects has recently been proposed as an alternative approach.4 However, studies of lung transplant for PAH-CHD are rare and have been limited to patients with Eisenmenger syndrome (ES). In a Nordic series of 63 transplanted ES patients, only 6 (9.5%) underwent double lung transplant, with survival comparable to that of patients undergoing heart-lung transplant.5 Similar results were reported in a recent American transplant registry of 442 ES patients, which also showed that posttransplant survival was independent of the type of defect.6 Our series is the first to include patients with distinct types of PAH-CHD and shows favorable progression in these patients, including those with previous sternotomy.
While acknowledging the limitations inherent to this type of study, we conclude that isolated double lung transplant is a valid option for PAH-CHD patients with simple or previously repaired defects. Double lung transplant in these patients is not accompanied by a higher rate of complications, and over the long-term resolves the cardiovascular symptoms with appropriate remodeling of the right cavities.
FUNDINGNo funding was received for the preparation of this article.
AUTHORS’ CONTRIBUTIONSAll authors contributed to the preparation of this article.
CONFLICTS OF INTERESTNone.