To the Editor,
The electrocardiographic criteria for ST-segment elevation acute coronary syndrome (STEACS) have not changed over time and the electrocardiogram remains the main diagnostic tool of this clinical disorder.
Thus, STEACS may be one of the most accurate clinical pictures for estimating differences in cardiovascular disease rates between different geographical locations or between different time periods in the same location. Recent studies suggest that hospitalizations for acute coronary syndrome have decreased in recent years due a reduction in hospitalizations for STEACS.1
The aim of the study was to identify differences in the incidence of hospitalizations for STEACS in our hospital over the past 20 years.
We determined the incidence of hospitalizations for STEACS in our hospital during the periods 1991-1993 and 2009-2010. The diagnostic criteria for STEACS used in both periods were persistent ST-segment elevation, increases and decreases in markers of myocardial damage, and chest pain or discomfort.
We only considered patients who were discharged to the cardiology unit from the intensive care unit (ICU) or directly admitted to the cardiology unit from the emergency department. This was because the information was obtained from the discharge reports for 2009-2010 and from the cardiology database for 1991-1993 and does not include patients who died in the ICU.
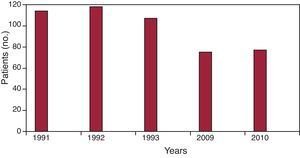
In the period 1991-1993, 339 patients were admitted with STEACS. During this period our hospital had a catchment of 234 000 individuals, representing an annual rate of 48.2/100 000 population. In 2009-2010, 152 patients were admitted with STEACS from a catchment area of 256 000 inhabitants, representing a rate of 29.6/100 000 population. The Figure 1 shows the number of hospitalizations.

Figure 1. Distribution of the number of patients hospitalized in the years analyzed.
The patients admitted in 2009-2010 were older, with a statistically significant difference between women. There were no differences in relation to sex, there were fewer anterior infarctions in the most recent period, and hospital stay has been reduced by approximately 1.5 days. The Table 1 shows the differences in the 2 periods analyzed and the conventional risk factors among the patients during the second period alone, as we cannot provide information about the first period.
Table 1. Differences in the Profile of Patients Hospitalized in the Two Periods and Conventional Risk Factors of Patients Included in the Second Period
| 1991-1993 (n=339) | 2009-2010 (n=152) | P | |
| Age, years | 64.11 (14.10) | 66.54 (13.47) | .070 |
| Older than 75 years, % | 21.2 | 28.3 | .080 |
| Women, % | 24.4 | 22.4 | .610 |
| Age of women, years | 70.7 (13.4) | 75.7 (10.9) | .040 |
| Age of men, years | 61.9 | 63.8 | .200 |
| Stay, days | 8.54 | 7.07 | .001 |
| Anterior location, % | 43.4 | 35.1 | .080 |
| First acute coronary event, % | 89.4 | ||
| Diabetes, % | 32.9 | ||
| Arterial hypertension, % | 53.3 | ||
| Hyperlipidemia, % | 38.2 | ||
| Smoking, % | 44.7 |
Unless otherwise indicated data are expressed as mean (standard deviation).
Our study shows a significant reduction in hospitalizations for STEACS in the last 20 years. Our data are consistent with the literature on other populations, albeit with significantly lower absolute numbers. A study conducted in California showed that the incidence of hospitalizations for STEACS, when adjusted for age and sex, decreased from 133 cases/100 000 inhabitants in 1999 to 50 cases/100 000 in 2008.1 Although we did not include patients who died in hospital before being transferred to the cardiology unit, if we take into account that the approximate mortality in the ICU in our hospital is 6%, the overall rate of hospitalizations would be approximately 53.6/100 000 population and 31.5%/100 000 population for the periods 1991-1993 and 2009-2010, respectively.
Although information is available on developments during the last decade of in-hospital mortality among patients with acute myocardial infarction in Spain,2 we have not found studies conducted by other Spanish hospitals or within the Mediterranean area that have used a methodology sufficiently similar to ours such that we can compare our results. However, some information can be obtained by extrapolating the available information on the epidemiology of ischemic heart disease in Spain. According to the rates of myocardial infarction observed in the MONICA-Catalonia, REGICOR and IBERICA studies, the estimated number of patients with acute myocardial infarction in Spain in 2002 was 68 494, of whom 59.8% (40 989) would have received hospital care.3 According to the MASCARA study,4 38% of patients hospitalized with acute coronary syndrome were cases of STEACS, such that in 2002, 15 575 patients with STEACS would have been hospitalized in Spain. If we take into account that at that time the Spanish population was 41 837 894, the estimated hospitalization rate would be 26.9/100 000, a Figure 1 similar to the one found in the present study.
Our study is limited by the fact that it was conducted in a single hospital, and thus we do not know if the results are applicable to other Spanish hospitals. In addition, as the patients who died in the ICU were not included, the total number of hospitalizations has been slightly underestimated, although we believe that the differences between the two periods would not be significantly different.
Hospitalizations for STEACS have decreased significantly in Spain in the past 20 years. The age of these patients has increased, particularly that of women. Anterior infarctions and mean stay have decreased. Our data show a trend similar to that presented in other populations, although with lower absolute numbers.
Received 20 December 2011
Accepted 25 January 2012
Corresponding author: vazquez89@arrakis.es