
Chagas disease is the first cause of nonischemic heart disease in Latin America and is associated with considerable morbidity and mortality.1 The prevalence of this condition has increased in Europe as a consequence of current migratory trends.2 Once the heart disease is established in this condition, there is no benefit from treating the infection.3 Hence, it is essential to achieve a prompt diagnosis to change the course and prognosis of the disease.
Natriuretic peptide analysis has shown diagnostic and prognostic value in several cardiomyopathies. Our aim was to achieve prompt detection of Chagas cardiomyopathy by analyzing the N-terminal pro-B-type natriuretic peptide (NT-proBNP), evaluating several echocardiographic parameters of diastolic dysfunction and systolic function, and determining the regional systolic shortening by myocardial strain measurement.
A prospective, observational study was carried out in 85 patients with positive serology for Trypanosoma cruzi between January 2015 and June 2016. All patients underwent NT-proBNP determination by chemiluminescence immunoassay, electrocardiography (ECG), and transthoracic echocardiography (TTE). In patients with abnormalities, cardiac magnetic resonance (MR) imaging was additionally performed.
The statistical analysis used SPSS v.21. Correlations of NT-proBNP concentrations with the ejection fraction and diastolic dysfunction parameters (mainly the indexed atrial volume and the E/e’ ratio) were analyzed using the Pearson test. The sensitivity and specificity of NT-proBNP for predicting Chagas cardiomyopathy was evaluated using a cutoff value of > 125 pg/mL, and the various echocardiographic parameters were compared after the patients were divided into 3 disease groups.
In our cohort, 95.3% were from Bolivia, 74.1% were women, and the mean age was 43 (range, 18-63) years. From the clinical viewpoint, 62.4% of the patients were asymptomatic. The most commonly reported symptom was palpitations in 25.9% of patients; only 9.5% were in New York Heart Association (NYHA) functional class ≥ 2. All patients had normal renal function and none were receiving treatment for heart failure at the time of inclusion.
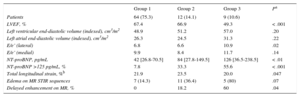
Patients were classified into 3 disease groups based on their characteristics: group 1 (indeterminate phase, positive serology with no abnormalities on ECG or TTE, n = 64); group 2 (2 or more of the ECG changes typically seen in Chagas disease, with normal TEE findings, n = 12), and group 3 (left ventricle dilatation, systolic dysfunction or segmental contractility abnormalities of the left or right ventricle on TTE; n = 9) (Table). Patients with Chagas cardiomyopathy were those in groups 2 and 3.
Main Variables by Groups
| Group 1 | Group 2 | Group 3 | Pa | |
|---|---|---|---|---|
| Patients | 64 (75.3) | 12 (14.1) | 9 (10.6) | |
| LVEF, % | 67.4 | 66.9 | 49.3 | < .001 |
| Left ventricular end-diastolic volume (indexed), cm3/m2 | 48.9 | 51.2 | 57.0 | .20 |
| Left atrial end-diastolic volume (indexed), cm3/m2 | 26.3 | 24.5 | 31.3 | .22 |
| E/e’ (lateral) | 6.8 | 6.6 | 10.9 | .02 |
| E/e’ (medial) | 9.9 | 8.4 | 11.7 | .14 |
| NT-proBNP, pg/mL | 42 [26.8-70.5] | 84 [27.8-149.5] | 126 [36.5-238.5] | < .01 |
| NT-proBNP >125 pg/mL, % | 7.8 | 33.3 | 55.6 | < .001 |
| Total longitudinal strain, %b | 21.9 | 23.5 | 20.0 | .047 |
| Edema on MR STIR sequences | 7 (14.3) | 11 (36.4) | 5 (80) | .07 |
| Delayed enhancement on MR, % | 0 | 18.2 | 60 | .04 |
LVEF, left ventricular ejection fraction; NT-proBNP, N-terminal pro-B-type natriuretic peptide; MR, magnetic resonance; STIR, short tau inversion recovery.
Values are expressed as No. (%) or median [interquartile range], unless otherwise indicated.
NT-proBNP values showed significant correlations with left ventricular ejection fraction and end-diastolic volume (r = -0.48 and 0.54 respectively; both, P < .001) and with diastolic dysfunction parameters, such as left atrial volume, the medial E/e’ ratio, and particularly, the lateral E/e’ ratio (r = 0.50, r = 0.62, and r = 0.83; P < .001 for the 3 parameters). The area under the ROC curve of NT-proBNP for detecting diastolic dysfunction (using the E/e’ ratio) was 0.92. However, 73.7% of patients with Chagas cardiomyopathy had a normal diastolic filling pattern.
NT-proBNP values in our sample showed no relationship with the values obtained in the analysis of myocardial deformation. There were no significant differences in myocardial strain values between patients with heart disease (groups 2 and 3) and those without (group 1).
NT-proBNP level was > 125 pg/mL in 9 of the 21 patients with Chagas cardiomyopathy (including abnormal TEE or ECG findings) (sensitivity, 42.9%). In group 1 (indeterminate phase), 7.8% of the patients had values above the reference range (specificity, 92.2%). The positive and negative predictive values of NT-proBNP alone for detecting Chagas cardiomyopathy were 64.3% and 83.1%, respectively. In some studies, the cutoff for women older than 55 years is > 150 pg/mL; at this level there would be an even greater decrease in sensitivity. The overlapping of the various diagnostic tests is depicted in Figure.

In endemic regions with limited resources, screening is still based on ECG and chest radiography findings. If this approach had been used in our cohort, 44.4% (4 of 9) of patients who had normal results on these tests, but had abnormal findings on TEE, would not have been diagnosed. By including NT-proBNP results, the diagnostic sensitivity would have improved. Only 22.2% (2 of 9) of patients would have been missed (50% relative reduction in false-negatives, although the number is small in absolute terms).
In patients in groups 2 and 3 who underwent cardiac MR imaging (n = 16), the most common findings were edema on short tau inversion recovery (STIR) sequences (50%), late enhancement (31.3%), and aneurysms (12.5%).
There was no association between myocardial strain and edema on MR imaging, which casts doubts on the diagnostic value of strain in the diagnosis of early phases of the disease.4
The practical conclusion of this study is that NT-proBNP is not sufficiently sensitive or specific to enable prompt detection of cardiac disease in low-risk patients in nonendemic areas. We believe that combined evaluation with ECG and TEE is required to achieve a greater diagnostic yield in the early phases of the disease.