To the Editor,
Unstable angina (UA) is a frequent cause of hospital admission. Risk stratification should be the first step in managing diagnosis and treatment.1 Nevertheless, despite the existing diagnostic resources, a substantial percentage of the patients that are at high risk according to the most widely used prognostic scoring systems (PSS) still show no evidence of coronary artery disease (CAD) in the angiographic study performed during the hospital stay.2..
With the aim of providing information to complement electrocardiography (ECG) and PSS in the management of these patients in the scenario described here, we studied whether variations within normal range (NR) in the levels of troponin I (TnI), measured serially in the emergency service using a conventional (as opposed to ultrasensitive) method, predicted the detection of CAD in the hemodynamic study...
For this purpose, we evaluated all the patients admitted to our service with UA in 2010. We included prospectively all the patients with no history of ischemic heart disease and a negative result in serial testing for enzymes indicative of myocardial damage, defined as levels below the 99th percentile of the upper reference limit (URL), associated with intermediate or high risk according to the Thrombolysis in Myocardial Infarction (TIMI) and Global Registry of Acute Coronary Events (GRACE) risk scores, who had undergone coronary angiography during the hospital stay. The final sample included 78 patients, with a mean age of 64.5 years. The study received the approval of the Ethics and Clinical Research Committee and all the patients signed the informed consent form...
At admission, the patient history and cardiovascular risk factors (CVRF) were recorded, as were the curves of the enzymes TnI and creatine kinase (CK), and the creatine kinase MB isoenzyme (CK-MB). The levels of these markers were determined by immunoassay using the UniCel® DxI 800 analyzer with the Access AccuTnI®, Synchron LX20® and Access CK-MB® kits, respectively (Beckman Coulter, Inc). An ECG finding of ST segment depression greater than 0.5mm and/or the presence of T wave inversion greater than or equal to 2mm in 2 or more contiguous leads was considered to be indicative of disease.3 The sample was divided based on the presence or absence of significant CAD in the hemodynamic study, defined as stenosis greater than 50% in left main coronary artery or greater than 70% in the remaining coronary arteries...
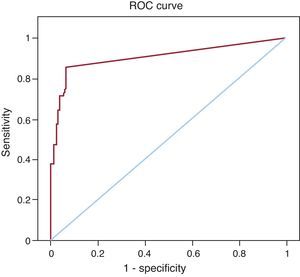
The patients with CAD presented higher peak TnI levels (0.098 ng/mL versus 0.012 ng/mL; P<.001; 99th percentile URL, 0.30 ng/mL); the distribution of the CVRF was homogeneous in both groups (Table). The analysis of the diagnostic yield of the percent increase in the TnI level within NR (between minimum and maximum values) for the detection of CAD had an optimal cut-off point of 20%. Thus, the highest percentages in the serial determination had a specificity of 95% and a positive predictive value of 96% in the diagnosis of CAD, with an area under the receiver operator characteristic (ROC) curve of 0.77 (95% confidence interval, 0.67-0.87; P<.001) (Figure) and an overall test accuracy of 70.6%. The positive likelihood ratio was 14.2...
Characteristics of the Sample According to the Presence of Coronary Artery Disease and After Application of the Optimal Cut-off Point of 20%.
| Characteristics | Sample | Without CAD | With CAD | P |
| Patients | 78 (100) | 24 (30.8) | 54 (69.2) | — |
| Age, years | 64.5±12.6 | 60.2±12.3 | 66.4±12.9 | .810 |
| Sex (men/women) | 44 (56)/34 (44) | 7 (34)/17 (66) | 37 (68)/17 (32) | .600 |
| Cardiovascular risk factors | ||||
| Hypertension | 56 (71) | 14 (58) | 42 (77) | .070 |
| Diabetes mellitus | 30 (38) | 8 (33) | 22 (40) | .530 |
| Dyslipidemia | 51 (65) | 17 (70) | 34 (63) | .500 |
| Smoking habit | 44 (56) | 13 (54) | 31 (57) | .790 |
| TIMI score | 3.19±1.16 | 3.00±1.06 | 3.28±1.20 | .190 |
| GRACE score | 115.21±29.39 | 107.71±25.72 | 118.60±30.51 | .300 |
| Hemoglobin, mg/dL | 13.3±1.7 | 13.1±1.3 | 13.4±1.6 | .770 |
| Creatinine, mg/dL | 1.1±0.8 | 0.9±0.2 | 1.1±0.3 | .890 |
| Disease-related electrocardiographic changes | ||||
| ST-T wave change | 34 (44) | 5 (21) | 29 (54) | .060 |
| Markers of myocardial necrosis | ||||
| Peak total CK, U/L | 118.1±86.1 | 11.1±70.7 | 129.4±114.6 | .650 |
| Peak CK-MB, ng/mL | 15±9.3 | 14.8±7.6 | 15.3±12.3 | .110 |
| %↑ CK-MB | 11.2±41.2 | 2.2±31.9 | 16.3±71.8 | .090 |
| Peak TnI, ng/mL | 0.071±0.090 | 0.012±0.005 | 0.098±0.009 | .001 |
| %↑ TnI | 94.2±218.4 | 2.1±10.3 | 139.4±323.2 | .001 |
| Characteristics | Sample | %↑ TnI <20% | %↑ TnI >20% | P |
| TIMI score | 2.24±1.20 | 2.21±1.20 | 2.27±1.20 | .830 |
| GRACE score | 115.8±29.4 | 115.5±26.6 | 116.1±33.7 | .940 |
| ST-T wave change | 34 (43) | 18 (36) | 16 (55) | .110 |
| %↑ CK-MB | 12±41.2 | 8.9±66.5 | 17.2±56.2 | .560 |
| %↑ TnI | 94.2±48.4 | 1.9±0.8 | 258±78.5 | .001 |
| CAD on coronary angiography | 54 (69) | 26 (53) | 28 (96) | .001 |
CAD, angiographically significant coronary artery disease; CK, creatine kinase; CK-MB, creatine kinase MB isoenzyme; GRACE, Global Registry of Acute Coronary Events; TIMI, Thrombolysis in Myocardial Infarction; TnI, troponin I measured by a conventional (as opposed to ultrasensitive) method; %↑, percent increase in serial measurements performed in the emergency service.
Data expressed as n (%) or mean ± standard deviation.

Figure. Receiver operator characteristic (ROC) curve corresponding to the diagnosis of coronary artery disease based on the percent increase in troponin I levels, within normal range, in serial measurements performed in the emergency service (optimal cut-off point, 20%).
Although to a great extent the ECG changes were able to distinguish the patients with CAD, the additional information provided by analysis of the TnI level significantly improved diagnostic specificity. We should point out that the PSS employed at the time of admission did not identify the presence of significant CAD...
We can conclude that, in the initial evaluation of the patient who is admitted for UA, analysis of the changes in TnI within the NR provides the clinician with supplementary information when establishing early invasive management due to its ability to predict angiographically significant CAD...
Diagnosis of UA is based on the combination of chest pain assessment and ECG changes and the determination of biomarkers. In the presence of the typical signs, with an estimate of intermediate or high risk according to the standard PSS, hospital admission is recommended for the purpose of evaluating the presence of CAD. In centers in which ultrasensitive TnI testing is not available, levels below the 99th percentile URL are considered to be a negative result, without taking into account in clinical practice changes in the concentrations that remain within this range. Previous studies have demonstrated the prognostic value of minor increases in TnI and the potential benefits of an early invasive strategy in patients with UA.4 While the consideration of TnI levels below the 99th percentile URL increases sensitivity in the diagnosis of CAD, it inherently involves a decrease in the specificity, although this can be improved by the combined analysis of temporal changes in TnI levels5 and the ECG findings. In our study, the percent change in these levels within NR was found to be an excellent tool for predicting CAD in the hemodynamic study, and it could orient clinicians to the invasive management of these patients...
The limitations of this study lie in the small sample size, the selection of patients who underwent coronary angiography during their hospital stay, and the need for a validation cohort that confirms the hypothesis we propose...
..
Corresponding author: osfan@comv.es