Calcified ostial lesions represent a challenge in coronary interventional procedures due to their rate of failure and complications. Coronary lithotripsy (CL), also known as coronary lithoplasty, is a technique that has recently come into use in the treatment of severely calcified coronary lesions.1,2 The technique generates rapidly expanding and collapsing bubbles inside the balloon, causing high-energy pulsatile sonic pressure waves that are transmitted through the balloon and produce microfractures in medial and intimal calcium deposits in the vessel wall.2 To our knowledge, there are no published cases specifically dealing with CL in severely calcified ostial lesions.
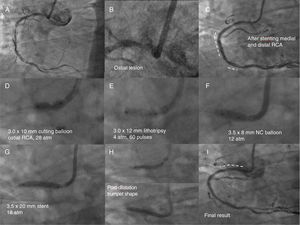
We present the case of a 62-year-old man, with a history of hypertension, diabetes, and stenting of the mid-right coronary artery (RCA) several years prior, who was admitted with progressive angina. Coronary angiography revealed a dominant RCA, with severe calcified ostial-proximal stenosis, severe restenosis of the stent in the mid-segment, and severe stenosis in the distal vessel (figure 1A-B). Predilatation was performed at several levels with a noncompliant (NC) balloon and a cutting balloon, followed by implantation of drug-eluting stents in the mid and distal RCA, with good result (figure 1C). However, several dilatations of the calcified ostial lesion were unsuccessful: initially, 3.0-mm NC balloons were used (which burst at over 24 atm), then a 3.0-mm cutting balloon with helical blades (inflated to 30 atm), and finally a 3.0-mm cutting balloon with axial blades (inflated to 28 atm), none of which expanded the lesion, and severe focal balloon underexpansion was observed (figure 1D). It was therefore decided to postpone the procedure for a second stage that could include either rotational atherectomy (RA) or CL; we decided to perform CL. Three days later, via a transradial approach and using a 6-Fr JR4 guide catheter, the ostial RCA lesion was dilated with a 3.0×12-mm CL balloon, inflated to 4atm in 3 sequences of 20 pulses each (figure 1E), followed by inflation to 6atm at the end of each sequence. The expansion of the lesion was checked with a single, low-pressure (12 atm) dilatation with a 3.5-mm NC balloon (figure 1F). Optical coherence tomography (OCT) and intravascular ultrasound (IVUS), both performed before and after CL, confirmed fractures at several points in the intimal plaque (and some in the medial layer), as well as a significant increase in the lumen area (figure 2A-C). Finally, a 3.5×20-mm drug-eluting stent was implanted at 18atm, positioned 1-2mm proximal to the aorto-ostial junction, and postdilated up to 20atm (with retraction of the balloon toward the aorta to create a trumpet-shaped flare), with an optimal angiographic result (figure 2G-I). Finally, IVUS confirmed the good result, with only slight underexpansion of the stent and no malapposed struts (figure 2A). No intraprocedural complications occurred, and 4 months later the patient was asymptomatic.
. The dashed lines in panels C and I mark the stented segments. NC, noncompliant; RCA, right coronary artery.")
Angiographic images of the RCA showing a severely fibrocalcified ostial plaque, stent restenosis in the mid segment and severe stenosis in the distal segment, and the sequence of treatment (explanatory labels in each image). The dashed lines in panels C and I mark the stented segments. NC, noncompliant; RCA, right coronary artery.
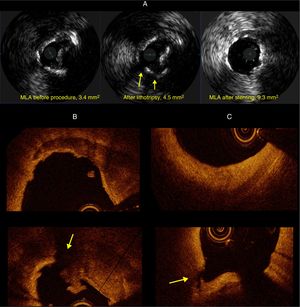
. C: image of fibrous plaque located 10mm distally, before and after lithotripsy. The arrows indicate areas of plaque rupture. MLA, minimum luminal area.")
A: intracoronary ultrasound images of calcified ostial plaque before and after lithotripsy, and after stenting. B: optical coherence tomography showing detailed images of the calcified ostial plaque before and after it was fractured with lithotripsy (with an image of a thrombus over the ruptured plaque). C: image of fibrous plaque located 10mm distally, before and after lithotripsy. The arrows indicate areas of plaque rupture. MLA, minimum luminal area.
Aorto-ostial lesions are usually more fibrotic and calcified, and they have a greater tendency to recoil.3 Several techniques have been used to try to modify these plaques prior to stenting: NC balloons, cutting balloons, and various atherectomy techniques, in particular RA and more recently orbital atherectomy. All of them are associated with an increased risk of coronary dissection and perforation.
Initial experience with CL has shown it to be safe and effective in the treatment of calcified coronary lesions.1,2 It may be preferable to RA in relatively large arteries (as in RA, a burr-to-artery diameter ratio> 0.7 is not advised) or when there is deep calcification. In addition, RA and orbital atherectomy of calcified ostial lesions have inherent technical difficulties and require relative coaxial alignment of the guide catheter with the artery, as well as careful handling of the guide catheter and ablation material (burr or crown). If the guide catheter is retracted too much, it may provide insufficient support for the device to cross the ostial lesion, and it may cause an unintended looping of the device (whipping) in the aorta and possible dissection. Early activation of ablation before the guide catheter has been sufficiently retracted can cause the material of the guide catheter itself to fragment and embolize. In contrast, CL is a simple technique that does not require special training and can be used in large arteries provided that the balloon-to-artery ratio is 1:1. The main limitations are that it is difficult for the device to cross critical stenoses, it requires a guide catheter ≥ 6 Fr, and currently there are no CL balloons available with a diameter> 4mm.
In reporting this case we have shown that LC is feasible in aorto-ostial calcified lesions and that it is a particularly effective tool in cases of severe calcification in which cutting balloon has been unsuccessful and other techniques such as atherectomy are unsuitable.
.