Balloon aortic valvuloplasty (BAV) has re-emerged as the treatment of choice for patients with severe aortic stenosis requiring urgent intervention, as a bridge to surgical or percutaneous (transcatheter aortic valve implantation [TAVI]) management, or as palliative therapy. This procedure has been traditionally performed via the femoral artery, requiring large-caliber sheaths that could lead to important vascular complications. Furthermore, femoral access is not always feasible due to severe iliofemoral disease. Consequently, the radial approach has arisen as a feasible option for BAV. Radial BAV have been reported using a low-profile, semicompliant balloon with an 8-Fr sheath with optimal results.1–3 Nevertheless, the radial diameter does not always allow the use of an 8-Fr sheath; moreover, valvuloplasty balloons that fit smaller Fr sheaths are not currently available.
We present a case of BAV performed via a bilateral (6-Fr) transradial approach. Informed consent to report this case was obtained from the patient, an 84-year-old man with an active, independent life, and a history of hypertension, diabetes, and obesity. He presented with symptomatic severe aortic stenosis and mild aortic regurgitation, with a mean gradient of 41mmHg, aortic valve area 0.87 cm2, and left ventricular ejection fraction of 40%. A coronary angiogram showed severe midleft anterior descending artery stenosis. The decision of the Heart Team was elective surgical aortic valve replacement and arterial graft bypass to the left anterior descending artery.
Weeks later, the patient was admitted with pulmonary congestion and mild left ventricular dysfunction. After deliberation by the Heart Team, it was decided to perform percutaneous revascularization of the left anterior descending artery with a drug-eluting stent and TAVI was scheduled. One week after discharge, the patient was admitted with a new episode of pulmonary edema and severe left ventricular dysfunction (ejection fraction 30%) requiring sedation, ventilatory support, intravenous vasoactive agents, and diuretics.
Following discussions with the Heart Team and considering the high bleeding risk (HAS-BLED, 4) and mild aortic regurgitation, it was decided to perform a bilateral transradial artery BAV guided by transoesophageal echocardiography. With the patient under general anesthesia, bilateral radial access was obtained with two 6-Fr sheaths. Temporary pacing was advanced via a 6-Fr right femoral venous access placed into the right ventricle, and hemodynamic monitoring was obtained with a pigtail catheter through a 6-Fr sheath inserted into the right femoral artery.
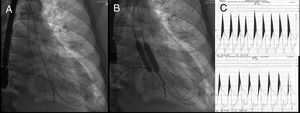
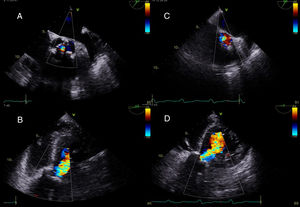
Two 275-cm preshaped TAVI (SAFARI2, Boston Scientific Co, Massachusetts, United States) guidewires were advanced via the bilateral radial artery, across the aortic valve into the left ventricle (Figure 1). Two Armada 35 (Abbot Vascular, Chicago, United States) angioplasty balloons, measuring 10 × 40mm and 12 × 40mm, were placed across the aortic valve, and simultaneous balloon dilatation was performed under rapid ventricular pacing at 160 beats per minute (Figure 1). Hemodynamic measurements demonstrated a reduction in the aortic valve gradient from 70 to 50mmHg after balloon valvuloplasty (Figure 1). Nonetheless, aortic regurgitation increased to moderate and so no further dilatation was performed (Figure 2). Radial sheaths were removed, and hemostasis was achieved with radial artery compression devices. Femoral hemostasis was achieved with an Angio-Seal 6-Fr vascular closure device.
 angioplasty balloons within the aortic annulus. C: hemodynamics: top, pre-BAV aortic gradient; bottom: post-BAV aortic gradient (19mmHg reduction). BAV, balloon aortic valvuloplasty.")
Fluoroscopy. A: transitory pacemaker placed in the right ventricle and two 275cm high support, preshaped guidewires in the left ventricle. B: deployment of 10 × 40mm and 12 × 40mm Armada 35 (Abbot Vascular, Chicago, United States) angioplasty balloons within the aortic annulus. C: hemodynamics: top, pre-BAV aortic gradient; bottom: post-BAV aortic gradient (19mmHg reduction). BAV, balloon aortic valvuloplasty.

After the BAV, the patient improved significantly, with reduced pulmonary congestion, and we were able to withdraw the vasoactive agents. Forty-eight hours later, TAVI was performed in the cardiac catheterization laboratory. The patient was under general anesthesia, and the right femoral artery was accessed for TAVI insertion. A 34-mm Evolut R valve (Medtronic Inc, Minneapolis, United States) was successfully deployed under controlled pacing, with no residual gradient and mild aortic regurgitation.
This case highlights the safety and feasibility of the bilateral transradial approach with 6-Fr sheaths for BAV in a patient with high bleeding risk and urgent need of afterload reduction as a bridge for TAVI in whom it was desirable to avoid the risk of femoral bleeding.
Vascular complications are the most frequent adverse events in this setting.4 As BAV is increasingly performed, it is essential to reduce the risk of femoral complications as much as possible. Thus, the bilateral radial artery approach using smaller caliber sheaths and double balloon angioplasty should be considered as the first choice irrespective of the presence of optimal vascular anatomy, as it might have 2 important benefits: a) to reduce upper-limb arterial complications, and b) to retain femoral access for TAVI.
.