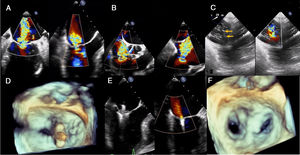
We present the case of an 84-year-old woman with a history of atrial fibrillation who was admitted to our hospital with heart failure and signs of systemic and pulmonary congestion. On admission, echocardiography showed severe mitral regurgitation (MR) due to annular dilatation and loss of leaflet coaptation, and torrential tricuspid regurgitation (TR) due to annular dilatation. Before a treatment decision was made, transesophageal echocardiography (TEE) was performed, showing a small coaptation defect between the A2-P2 scallops of the mitral valve (figure 1A, video 1 of supplementary data, and at the tricuspid valve there was loss of coaptation along the line between the anteroseptal and posteroseptal commissures, more marked centrally, causing a torrential TR jet (figure 1B,C, video 2 of supplementary data).
. D: 3D TEE showing clip at the mitral valve. E: TEE of insertion of leaflets in the clip and result. F: 3D TEE of the mitral clip final result. TEE: transesophageal echocardiography.")
A: TEE showing severe mitral regurgitation. B: TEE mid-esophageal view of the torrential tricuspid regurgitation. C: TEE showing gaps along the line between the anteroseptal and posteroseptal commissures (arrows). D: 3D TEE showing clip at the mitral valve. E: TEE of insertion of leaflets in the clip and result. F: 3D TEE of the mitral clip final result. TEE: transesophageal echocardiography.
During discussion between medical and surgical teams, the case was considered to be high risk, and conventional surgery was ruled out. Given the poor response to medical treatment, combined treatment using MitraClip (Abbott Vascular, USA) was planned. The procedure was carried out under general anesthetic with fluoroscopy and TEE guidance.
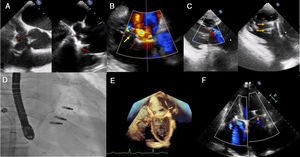
First, after transseptal puncture, a MitraClip NTR system was advanced toward the mitral valve, and 1 clip was implanted centrally, reducing the MR from 4+to 1+(figure 1D-F). Next, the guide catheter was withdrawn to the right atrium. Using the modified Munich technique, 2 XTR clips were implanted to capture the anterior and septal leaflets, reducing the TR from torrential to moderate (figure 2a-d, video 3 of supplementary data).
. B: TEE of the first (red arrow) and second (yellow arrow) clips. C: transgastric view TEE on long and short axes, final result in color, and visualization of the 2 clips (yellow arrows), respectively. D: fluoroscopic images. E: 3D TTE; mitral clip (green asterisk) and tricuspid clip (red asterisk). F: TTE of the result at follow-up. TEE, transesophageal echocardiography; TTE, transthoracic echocardiography.")
A: TEE showing the clip in the center of the valve, with its arms open onto the leaflets (red arrows). B: TEE of the first (red arrow) and second (yellow arrow) clips. C: transgastric view TEE on long and short axes, final result in color, and visualization of the 2 clips (yellow arrows), respectively. D: fluoroscopic images. E: 3D TTE; mitral clip (green asterisk) and tricuspid clip (red asterisk). F: TTE of the result at follow-up. TEE, transesophageal echocardiography; TTE, transthoracic echocardiography.
The patient progressed well and was discharged at 48hours. At 5 months post-procedure, she was stable, in New York Heart Association functional class II, and had had no readmissions. Transthoracic echocardiography showed good biventricular function, with mild MR and moderate TR, with no pulmonary hypertension (figure 2E,F, video 4 of supplementary data).
Tricuspid regurgitation often occurs along with MR. According to the clinical guidelines, and from a surgical point of view, when both conditions are present at diagnosis, concomitant treatment of the tricuspid valve should be considered, as it improves long-term outcomes.1 In recent years, growing use and advances in percutaneous treatment of the mitral valve have shown it to be a safe and effective strategy in patients with primary and secondary MR.2 Successful tricuspid repair with this device has also been described.3 However, there is little information on percutaneous repair of both valves in a single procedure. One of the main advantages of transcatheter treatment is that the procedures can be staged, allowing assessment of the right valve disease after correction of the left. However, combined treatment has been reported to be safe and may even be associated with better prognosis compared with isolated mitral valve repair.4 Nonetheless, this approach requires a longer procedure and the technique is more demanding. Furthermore, TEE imaging adds complexity in cases involving the tricuspid valve, for which acquisition of high-resolution images can represent a challenge.5
This case supports the feasibility of this procedure. As described in other series,3,4 it resulted in improvement in functional class and reduction in TR, which can be considered successful given the patient's initial status. However, it is still difficult to decide which patients should be treated simultaneously and which should receive mitral treatment and await a decision on tricuspid intervention based on the procedural outcome. Probably, patients with a long history of atrial fibrillation, severe atrial and annular dilatation, and coaptation defects would be candidates for combined treatment in a single procedure. However, more studies are needed to define this profile more clearly.
In conclusion, percutaneous mitral and tricuspid repair in the same procedure with the MitraClip device is a safe and feasible strategy and can improve quality of life and functional class in this subgroup of patients.
CONFLICTS OF INTERESTR. Estévez-Loureiro is a proctor for MitraClip ad has received fees from Abbott Vascular. E. Abu-Assi is associate editor of Revista Española de Cardiología; the editorial procedures established by the journal have been followed to ensure the impartial management of this manuscript. The other authors have no conflicts of interest.
Supplementary data associated with this article can be found in the online version available at https://doi.org/10.1016/j.rec.2020.05.031