
To the Editor,
.
Castleman disease, or angiofollicular lymph node hyperplasia, is a rare lymphoproliferative disorder of unknown etiology and pathogenesis. Its importance lies in the fact that it has been associated with human immunodeficiency virus (HIV) and human herpes virus 8, as well as other neoplastic diseases such as Kaposi's sarcoma, lymphomas, and POEMS syndrome (polyneuropathy, organomegaly, endocrinopathy, M protein, and skin changes)..
We present the case of a 66-year-old man with no known cardiovascular risk factors who complained of dyspnea upon moderate exertion, together with a weight loss of 4 to 5 kg over a 6-month period. In the physical examination, a grade 2/6 systolic murmur was detected at the pulmonary site (left second intercostal space) on auscultation. A chest X-ray showed no evidence of cardiomegaly or signs of pulmonary congestion. Transthoracic echocardiography revealed the presence of mild pulmonary stenosis with a peak pressure gradient of 23mmHg and, on the parasternal short-axis view, there was a marked concentric thickening of the ascending aorta, which exerted pressure on the pulmonary artery. In view of the echocardiographic findings, we performed a magnetic resonance study (Figure 1, Figure 2), which revealed a soft tissue mass surrounding the aortic root and ascending thoracic aorta and occupying the lumen of the pulmonary trunk. The mass extended toward the right pulmonary artery, occupying its entire lumen and infiltrating the right atrium as well. Following the administration of an intravenous contrast medium, there was a marked enhancement of the mass that revealed the extensive vascularization of the lesion. Positron emission tomography/computed tomography was performed to rule out the existence of lesions at other sites. The patient was referred to cardiac surgery for resection of the mass. Following median sternotomy, the pericardium was opened and an infiltrative process involving the aortic root and ascending aorta, pulmonary trunk, and right atrium was identified. Because of the close proximity of the lesion to the great vessels, only partial resection was possible, concluding with layered closure using a Peri-Guard repair patch. The final pathology report concluded that the lesion consisted of a polyclonal lymphoid proliferation that was compatible with the plasma cell variant of Castleman disease. As the mass had only been partially resected, the decision was made to administer neoadjuvant therapy with the anti-CD20 monoclonal antibody, rituximab. The patient has responded favorably to treatment and 1 year later is asymptomatic. Follow-up computed tomography scans show a considerable reduction of the size of the mass. Any association of this case with HIV or with other neoplastic diseases was ruled out..

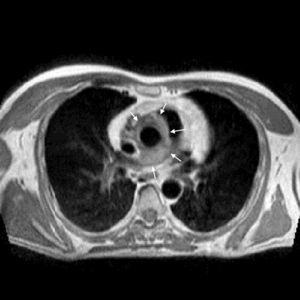
Figure 1. Axial “black-blood” magnetic resonance image showing a soft tissue mass surrounding ascending thoracic aorta, extending to and occupying the lumens of pulmonary trunk and right pulmonary artery (arrows).

Figure 2. Coronal “black-blood” magnetic resonance image showing a soft tissue mass occupying the entire right pulmonary artery lumen (arrows).
Castleman disease has two variants with highly different prognoses and treatments: multicentric and unicentric, the latter constituting 70% of the reported cases.1 The most common sites are chest (70%), neck, abdomen, retroperitoneum, and pelvis. Histological criteria define two types: the hyaline vascular variant (the more prevalent type) and the plasma cell variant (which accounts for only 10% to 20% of the cases)..
Unicentric Castleman disease is a generally benign disorder that is usually classified as belonging to the hyaline vascular type. It is found in young adults, and most of the patients are asymptomatic. In contrast, the multicentric form is found in older adults and is usually associated with the plasma cell variant, a systemic disease with generalized lymphadenopathy, hepatosplenomegaly, fever, and night sweats; in addition, it is frequently associated with HIV infection.2.
The treatment of choice of the unicentric form is surgical, and complete resection is curative in most cases. If the lesion cannot be resected completely, the prognosis with partial resection is also favorable, and the patient may remain asymptomatic for years. Other therapeutic options include preoperative embolization, radiotherapy, and chemotherapy. The experience with the use of rituximab in unicentric Castleman disease is limited, although there are reports of cases in which promising results were obtained in patients with unresectable disease or in whom partial resection was performed. In the multicentric form, surgical resection is not sufficient, and the association of radiotherapy and chemotherapy is necessary.3.
Castleman disease is a rare disorder, the diagnosis of which requires a high degree of suspicion, due to the absence of specific clinical or radiological findings; the definitive diagnosis is based on the pathological study. It should be considered in the differential diagnosis of any mediastinal mass.4.
Corresponding author: fj.garci@hotmail.com