Keywords
Received February 4, 2005. Accepted for publication May 13, 2005.
INTRODUCTION
Cardiac cephalgia was first defined as a separate entity in 1997.1 The authors of the study reported 2 personal cases and reviewed five previously published case studies of patients seeking medical advice for headache as a manifestation of myocardial ischemia, and proposed the term cardiac cephalgia. All 7 patients presented myocardial ischemia and headache on physical exercise, which disappeared with medical treatment or revascularization for ischemic heart disease. The International Headache Society has recently included "cardiac cephalalgia" as a specific entity in its international classification of headache disorders2 and proposed diagnostic criteria (Table).

Our aim is to draw attention in our setting to this novel entity, presenting the first 2 cases of cardiac cephalgia described in Spanish.
CASE STUDIES
Patient 1
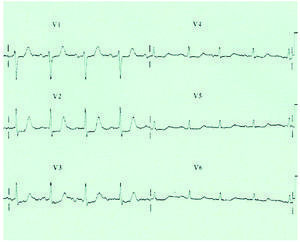
A 74-year-old woman was admitted to the neurology department of our hospital for incapacitating headache of 15 days' evolution. The patient had a history of ischemic stroke in 1985 (without sequelae), obesity, and oral antidiabetic therapy, but no migraines. Three months earlier she had presented a syncopal episode of 1 minute's duration, of unknown origin. Since then she had a sedentary lifestyle, restricted to her home. The patient was admitted for pulsating headaches lasting from a few minutes to several hours, occurring 1 to 4 times a day, located in both temples and accompanied by nausea. The routine analytical study, chest x-ray, electrocardiogram, and cranial computed tomography scans were normal; however, the episodes did not cease with paracetamol or ketorolac. On the third day, while in bed the patient reported a new episode of incapacitating headache accompanied by nausea, sweating, and a mild feeling of oppression in the middle chest. The ECG showed anterior ST segment depression (Figure). Both the headache and the electrocardiographic abnormalities abated rapidly with sublingual nitrates. Afterwards, creatine kinase and troponin I levels, which were normal at the time of admission, rose to 194 and 0.25 (normal values, 190 and <0.04, respectively). The patient experienced an identical event some hours later, but was asymptomatic following treatment with a 20-mg nitroglycerin patch.

Figure. Detailed view of the electrocardiogram for the first case during a headache episode in which ST segment depression was observed in V2 to V4. This descent disappeared after sublingual administration of nitrites.
Patient 2
A 64-year-old woman with a history of hypertension, diabetes, hypercholesterolemia, and ischemic heart disease (prior AMI) but no migraines, who was under insulin, aspirin, enalapril, furosemide, and simvastatin therapy, was seen for daily headaches on physical effort or that interrupted nighttime sleep. The headaches were severe, oppressive, usually one-sided and occasionally radiating to the jaw, with a typical duration of 1 hour; however, there was no chest pain, dyspnea, sweating, or abdominal discomfort. The examination, laboratory tests, and neuroimaging were normal. The patient had spontaneously observed that nitrites, which she was using for angina attacks, would cause the headaches to improve within a few minutes. She died suddenly 6 months after the onset of her headache episodes. Cardiac enzymes levels were never determined and no electrocardiograms were performed during the headache episodes.
DISCUSSION
The 2 patients described met the diagnostic criteria for cardiac headache since both presented concomitant episodes of myocardial ischemia and severe headache accompanied by nausea that abated after the administration of nitrates.1,2 This entity should be suspected in the case of any de novo headache beginning after age 50 in patients with vascular risk factors, in particular ischemic heart disease. The response to nitrates confirms the diagnosis. As observed in our patients, headache does not always occur at the same time as the typical chest pain of myocardial ischemia or only during effort. Similar to angina, cardiac cephalgia can occur at rest, as described by us in the first Spanish patient with this diagnosis.3 Cardiac cephalgia is considered an extremely rare entity; however, our own experience with three recent cases and the report of a growing number of patients in recent years4 suggest that this entity is more frequent than previously thought. This kind of headache typically goes unnoticed in the context of the more worrisome myocardial ischemic process or is misinterpreted as secondary to nitrates, since it is well known adverse event of this pharmacological group, particularly in patients who suffer from migraines. Recognition of cardiac headache is not a trivial issue and the differential diagnosis with migraine, a very similar type of headache, is crucial to prevent the administration of medications with vasoconstrictor capacity (e.g., ergotamines and triptans), contraindicated in patients with ischemic heart disease. Therefore, cardiologists should be familiar with the main diagnostic features of this entity.
Finally, the pathophysiological mechanism of this condition should be elucidated. Three theories have been proposed. The first suggests that cardiac cephalgia is referred pain, similar to what occurs in the shoulder with hepatic lesions, since there is a connection between the central cardiac pathway and the cranial pain afferents. The cardiac sympathetic fibers originate from the cervical lymph nodes, which also innervate pain-sensitive cranial structures.5 The second hypothesis proposes that the cephalgia is secondary to elevated intracranial pressure due to venous stasis caused by a transient decrease in cardiac output.6 Finally, it has been put forward that cardiac cephalgia may be secondary to the local release in the heart muscle of chemical mediators capable of inducing remote pain, in this case headache. Serotonin, bradykinin, histamine, and substance P have been proposed as potential pain-producing substances. The increase in intracardiac pressure during angina attacks could also result in a release of natriuretic peptides, which could induce headache due to a high capacity to dilate the cerebral vasculature.7-9
ACKNOWLEDGEMENTS
We would like to thank Dr. F. Sábada for his valuable assistance with the preparation of case 2.
Correspondence: Dr. J. Pascual Gómez.
Servicio de Neurología. Hospital Universitario Marqués de Valdecilla.
Avda. Marqués de Valdecilla, s/n. 39008 Santander. España.
E-mail: juliopascual@telefonica.net