Keywords
INTRODUCTION
Cardiac catheterization by radial artery access was described by Campeau1 in 1989 and later used by Kiemeneij et al2 in coronary interventional procedures. This technique has shown a low rate of vascular complications3; it allows early ambulation,4 is less costly,5 and favors the patient's well-being.5 Catheterization through the radial artery has gradually increased is Spain6 and is now used routinely in some centers.7,8
The radial artery possesses anatomic and functional characteristics, such as spasm,9,10 tortuosity,10 and congenital anomalies11 that can make it difficult to access. Its small diameter and inherent vascular reactivity require an attentive catheterization technique. Design improvements in the material involved have resulted in smaller diameters, which have led to a decrease in trauma to the artery. In addition, the use of a single catheter to perform several tasks permits a reduction in arterial manipulation.
Due to the anatomic relationship between the brachiocephalic trunk and the aortic arch, the Judkins left 3.5 catheter (JL 3.5) is often used to catheterize the left coronary artery using the right radial artery approach.12 The aim of this study was to: 1) determine the percentage of cases in which selective catheterization of both coronary arteries can be performed by radial access with a JL 3.5; 2) analyze the incidence of potential complications derived from this technique, and 3) determine whether there is an increase in the procedure time with this method as compared to use of a specific catheter for each artery.
PATIENTS AND METHOD
Design
Prospective cohort study performed at a single center.
Patients
A cohort of 100 consecutive patients referred for coronary angiography with right radial artery access was prospectively studied. Patients with aortic valve disease or revascularization treatment were excluded. The baseline characteristics, complications associated with the technique, and time interval from insertion of the introducing sheath to withdrawal of the last catheter were studied. In all cases a minimum of 4 views were taken of the left coronary and 2 of the right coronary, followed by left ventriculography with a pigtail catheter. The mean duration of the study was compared to that of a control group of 20 consecutive patients in whom a 6-Fr JL 3.5 was used for the left coronary and a 6-Fr Judkins right 4 catheter (JR 4) for the right coronary, followed by left ventriculography.
Catheterization Technique
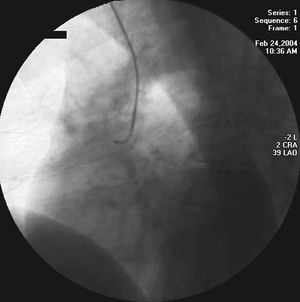
All procedures were performed by 2 experienced interventional cardiologists. After inserting a 12-cm, 6-Fr hydrophilic-coated Terumo™ introducing sheath (Radiofocus II, Terumo Corporation, Tokyo, Japan) 5000 units of heparin, 200 µg of nitroglycerin, and 1 mL of bicarbonate were administered. The left coronary was studied with a Cordis™ 6-Fr JL 3.5 catheter (Cordis Corp., Johnson & Johnson), and the tip was subsequently withdrawn to the ascending aorta. The rigid tip of the 0.035-inch guidewire was advanced to a point 2 cm from the distal orifice of the catheter. The primary curve of the catheter was rectified, such that the morphology of the JL 3.5 resembled that of a JR 4 (Figure 1), and selective catheterization of the right coronary artery was performed in a conventional manner (Figure 2). In cases in which the coronary could not be studied with a JL 3.5, a JR 4 was used. The procedure was completed with left ventriculography.

Figure 1. Judkins left 3.5 catheter with curve modified by the rigid tip of the 0.035 guidewire in the interior.

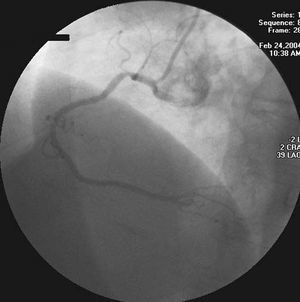
Figure 2. Contrast injection in the right coronary using a Judkins left 3.5 catheter.
Statistical Analysis
Continuous variables were expressed as the mean ± standard deviation and qualitative variables as percentage. Student t test was used to compare means and the χ² test to compare proportions. All values were analyzed bilaterally and P-values of ≤.05 were considered significant. The results were analyzed with SPSS 12.0 for Windows.
RESULTS
A total of 100 consecutive patients were included in the study. Baseline characteristics and indications for the procedure are shown in Table 1.

Both coronaries were selectively catheterized with the JL 3.5 in 94% of the cases. In 6 patients a JR 4 was required for catheterization of the right coronary, 5 because of technical problems and 1 because of severe spasm at the origin of the right coronary due to excessively deep intubation. There were no cases of radial artery spasm (Table 2). The time required for the procedure in this series was not significantly longer than that of the control group (16.9±6.9 vs 15.8±6.7 min; P=NS).

DISCUSSION
The main finding of this study is the feasibility of using a single 6-Fr JL 3.5 catheter to study both coronary arteries in the majority of cases, with a small incidence of radial spasm or other complications and without increasing the procedure time.
With the technique described, there is less manipulation of the radial artery because fewer catheters are used. Although the technique is simple to perform, several aspects should be considered to prevent potential complications. When performing the procedure, an attentive technique is absolutely essential. There were no serious complications in our study, however the number of patients studied was limited, and therefore the less frequent complications may not have presented themselves. Among the points to consider, one must assure that the catheter is withdrawn to the ascending aorta and is outside the origin of the trunk before inserting the rigid tip of the guidewire. The guidewire tip must never prolapse outside the catheter, since potential trauma to the ascending aorta, aortic valve, or origin of the coronary arteries could have fatal consequences. It is also important to keep in mind that the preformed curve of the JL 3.5 gives the catheter an inherent tendency to enter the conus artery or to advance deeply into the origin of the right coronary, with the risk of an aggressive impact that could lead to dissection of the vessel. Hence, it is important to confirm the position of the catheter and always examine the pressure recording before starting the injection. With due attention to these factors, the technique is fast, simple, and safe.
The study was performed with 6-Fr catheters because they are the ones routinely used in our center. Nevertheless, the purpose of the study was to determine the feasibility of the technique; hence it could be performed with smaller catheters. The choice of diameter depends on the criteria of the angiographer. The 6-Fr catheter may have the advantage of easier manipulation and better image quality in some cases, as well as provide the possibility to perform techniques such as atherectomy, intracoronary ultrasonography, thrombectomy, or interventional procedures on junction lesions.3 In addition, as compared to 4-Fr catheters, it does not require changing the sheath when an interventional procedure is decided during the same procedure. This situation occurred in only 5% of patients in our series, but may be more frequent in other settings. The 6-Fr catheters would be especially useful in patients with acute myocardial infarction, who are likely to require angioplasty. Nevertheless, the diameter of 6-Fr catheters is often larger than that of the radial artery, a fact that would induce spasm, which is precisely the most frequent complication of this technique. Although the incidence of this complication has decreased, it develops in 10%10 of cases and can reach 30% if preventive measures are not taken.13 The importance of radial spasm lies in its repercussion on the patient's well-being,13,14 its influence on the success of the procedure,13,14 and the triggering of a loss of pulse at the end of the procedure.15 In sporadic cases, extraction of the radial artery15,16 or fragmentation of the access sheath within the artery have occurred.17
The cases included in our series were diagnostic; however, 5 of our patients underwent a percutaneous intervention in both arteries during the same procedure, using of a 6-Fr JL 3.5 Cordis Brite Tip® (Cordis Corp. Johnson & Johnson) in all cases. The origin of the right coronary artery is located anterior to the brachiocephalic trunk, and the proximal segment of the artery runs in an anteroposterior direction.17 This soft-tipped catheter allows deep intubation with satisfactory support and no trauma to the coronary. In fact, once it is inserted in the ostium, the positioning of the device strongly resembles that of Ochiai's catheter specifically designed for use in the right coronary by radial access.18
Lastly, one of the advantages of the radial approach is the cost savings,19 mainly derived from earlier ambulation. Use of a single catheter for both diagnosis and interventional therapy allows for a slight additional savings. As seen from the results of this study, the technique did not involve an increase in the duration of the procedure.
LIMITATIONS
The number of cases in our series was limited, therefore the potential development of infrequent but important complications, such as dissection at the origin of the right coronary, could not be reliably evaluated. Determination of the length of the procedure was done by comparing with a control group in a non-randomized manner; therefore, possible bias associated with this type of design cannot be ruled out. A prospective, randomized study is necessary to confirm this finding.
Lastly, patients with aortic valve disease or prior revascularization surgery, who often present the greatest difficulty in radial catheterization, were excluded.
CONCLUSIONS
Cardiac catheterization using a JL 3.5 catheter and right radial artery access permits the study of both coronary arteries in a large percentage of cases, involving a low incidence of complications and a slight reduction in costs due to the cutback in the number of catheters required. The decrease in radial artery manipulation with the limited passage of catheters may prevent radial spasm without increasing the time required for the procedure. Randomized studies are needed to confirm these last two aspects.
Correspondence: Dr. I. Lozano.
Instituto, 7, 2.o dcha. 33201 Gijón. Asturias. España.
E-mail: imlml9@hotmail.com