Keywords
INTRODUCTION
According to the literature, some 5%-15% of patients with transposition of the great arteries have their coronary arteries arising from the same aortic sinus (CASS). The difficulty this causes when trying to transfer the coronary arteries to the neoaorta without distorting them means such anatomy is associated with increased surgical risks.1-5 The transfer technique needs to be individualized depending on the vascular arrangement and the relationship between the initial section of the coronary arteries and the great vessels. Coronary arteries arising from the same aortic sinus may have a single ostium (often referred to as a "single coronary artery") or 2 independent ostia. Generally they arise from sinus 2 (posterior right). It is common for the epicardial route taken to be unusual, and the left coronary artery may have an intramural trajectory, which increases the risk of causing it injury.4 In CASS arising from a single ostium, the coronary arteries have a common trunk and all 3 run on the same side of the aorta; normally none of them run between the aortic and pulmonary artery roots. This means they can all be transferred as a single button using the trap door technique with excellent results.6
Transfer surgery in patients with 2 separate coronary arteries that arise from a single sinus is more complicated since one of the arteries crosses between the aorta and pulmonary artery, commonly with an intramural trajectory. Thus, the coronary arteries pass on either side of the pulmonary artery root and impede the surgical rotation of the coronary button for its reimplantation in the neoartoa. Patients with this anatomy suffer a higher mortality rate.4 On some occasions, if the distance between the ostia is sufficient, the coronary arteries can be separated so that they can be reimplanted independently using the usual technique.7 In other cases the aortocoronary flap technique offers excellent results, even in patients in whom the trajectory of the left coronary artery is intramural.6,8,9
METHODS
Since 2001, 3 patients with transposition of the great arteries plus CASS showing separate coronary arteries have undergone surgery at the Cardiovascular Surgery Unit of the Hospital Reina Sofía in Cordoba. Table 1 shows their pre- and postoperative data. The first patient underwent the independent reimplantation of each coronary artery following the normal technique. In the second and third patients, the aortocoronary flap technique was followed.

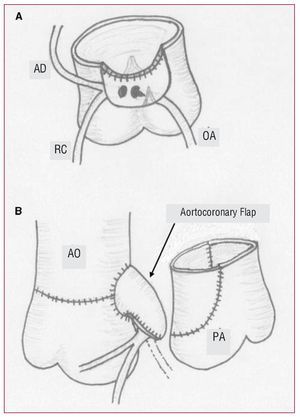
To make the aortocoronary flap, the origin of the coronary arteries was dissected out as a single wide button, avoiding any damage to the left coronary artery following an intramural trajectory. This required the deinsertion of the posterior commissure of the aortic valve. If the ostium of the intramural coronary artery shows any stenosis, this should be corrected by resecting a wedge of tissue from the wall of the aorta that forms the edge of the orifice, following the technique of Mee.7 The upper part of the coronary button was sutured to the anterior zone of the neoaortic root, without rotating the coronary arteries, and the anterior face of the connection was reconstructed with pericardium (Figure 1).

Figure 1. Surgical technique used with patient 3. A: preparation of the coronary button to be sutured to the upper border of the neoaorta without rotating or displacing the coronary arteries. The deinsertion zone of the aortic commissure can be seen, as well as amplification of the left coronary artery ostium. B: appearance of the aortocoronary flap (arrow) after completing the connection with the patient's own pericardium, and its relationship with the pulmonary artery root. AD indicates anterior descending artery; Ao, aorta; Cx, circumflex artery; Pa, pulmonary artery; RC, right coronary artery.
RESULTS
In the first patient, who had a single ostium for the DA-Cx and another for the CD (2LCx-R), each ostium was transferred independently of the neoaorta. The patient suffered severe ischemic ventricular dysfunction, which prevented the disconnection of the extracorporeal circulation, even though the revascularization of the left coronary artery was attempted using a mammary bypass.
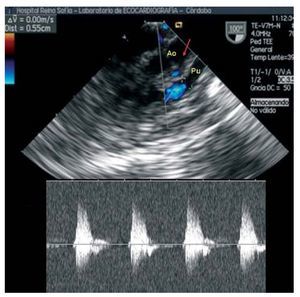
In the other 2 patients, who showed a common ostium for the CD-Cx and an intramural exit of the DA (2L-CxR), the coronary arteries were transferred using an aortocoronary flap. Both patients progressed well. One patient who showed closure of the ventricular-septal defect required the implantation of a definitive DDD epicardial pacemaker via left thoracotomy owing to persistent postoperative atrioventricular block. Postoperative and follow-up echocardiograms of these two patients showed normal biventricular function and normal flow at the aortocoronary connection (Figure 2). No angiographic monitoring was performed.

Figure 2. Echographic image (transesophageal) of the aortocoronary connection between the aortic root and the pulmonary artery (arrow) in patient 3. Pulsed Doppler analysis showed a normal systolic flow coming from the aorta in the aortocoronary flap.
DISCUSSION
The main cause of early death in patients who have undergone arterial switch is myocardial ischemia owing to technical problems encountered during coronary reimplantation. The origin of the coronary arteries in a single aortic sinus is an important risk factor, despite the development of techniques designed to deal with such cases. In addition, the coronary arteries of such patients commonly take unusual epicardial routes and have intramural trajectories, making their transfer even more risky. Although in the past some authors recommended treating such patients via physiological correction (atrial switch),10 it is now accepted that all coronary artery patterns can be transferred with acceptable risk if the right technique is used.11 Nonetheless, a meta-analysis by Pasquali et al.4 shows that the existence of a "single coronary artery" (odds ratio [OR]=2.9) and, especially of an "intramural coronary artery" (OR=6.5) have persisted as risk factors over the last 2 decades. The term "intramural coronary artery" includes any pattern in which the coronary arteries cross between the great vessels, which we have here termed CASS.
Numerous techniques have been described for the reimplantation of the coronary arteries in patients with CASS. In patients in whom the initial courses of the coronary arteries do not lie on either side of the pulmonary artery root (when there is a single ostium) the trap door technique provides excellent results.6 Some authors recommend the use of pericardial patches in the reimplantation of coronary arteries with a single ostium.12 When there are 2 independent coronary arteries, one (normally the left) runs between the aorta and pulmonary artery and commonly has an intramural trajectory; the arteries therefore pass on either side of the pulmonary artery root. In such cases, 2 transfer techniques can be used13:
- Separating the coronary arteries and transferring them independently, following the normal technique
- Maintaining the arrangement of the coronary arteries, obtaining a single button and creating a para-aortic connection either directly8 or using a pericardial patch (Quaegebeur JM, personal communication, 1992)
The main problem of separating coronary buttons is the lack of tissue for suturing without leaving any stenosis of the ostium. Although some authors report good results,7 others have reported frequent coronary complications, as shown by the first of our 3 patients.6
Using an aortocoronary flap avoids rotating the aortic button that includes the origin of the 2 coronary arteries, and therefore reduces the risk of their distortion. However, the risk of compressing the aortocoronary connection between the aorta and pulmonary artery exists. This risk is low if the pulmonary arteries are adequately mobilized, but it may be necessary to displace the distal pulmonary anastamosis towards the right or left pulmonary artery. Another cause for concern with this technique is the possibility of the retraction or degeneration of the pericardial patch obstructing the coronary flow.
Different techniques have been described for keeping the coronary arteries in situ, involving an intrapulmonary tunnel with pericardium connecting the coronary ostia to an "aorto-pulmonary window,"14 or via aortic wall flaps that create an aorto-coronary connection within the neopulmonary root.15-17 However, experience with these techniques is limited.
The results obtained with the present patients treated using the aortocoronary flap technique were satisfactory, while the patient who underwent independent transfer of the coronary arteries died due to myocardial ischemia. Thus, we believe it is safer to transfer separate coronary arteries that arise from a single sinus via the use of a single button, except in exceptional cases when there is sufficient distance between the coronary ostia.
Correspondence: Dr. C.M. Merino Cejas.
Martín de Saavedra, 9. 14012 Córdoba, España.
E-mail: cmmerinomjmolina@hotmail.com
Received November 29, 2007.
Accepted for publication February 11, 2008.