Although we know that dyslipidemia is one of the major cardiovascular risk factors, especially with regard to myocardial infarction,1 and that the strict control of lipid concentrations, specifically that of low-density lipoprotein cholesterol (LDL-C), is associated with a reduction of cardiovascular events,2,3 the fact is that true control is very far from optimal.4 In the CODIMET study,5 we demonstrated that over 80% of the high risk patients in Spain fail to meet the LDL-C criteria recommended by clinical practice guidelines.6 The aim of this analysis is to determine whether there are differences in the control of LDL-C depending on the medical specialty and Spanish autonomous community.
CODIMET is a multicenter, cross-sectional, observational, epidemiological study involving retrospective data collection over the 3 months prior to the inclusion of the patient or during the study visit. There were no changes in patient management. The participants were 874 Spanish specialists in cardiology, endocrinology, internal medicine, or primary care. This sample is representative of the types of physicians involved in the care of this Spanish population. We included patients of both sexes, over 18 years of age, with at least one prior episode of acute myocardial infarction or angina pectoris (coronary group) or diagnosed as having type 2 diabetes mellitus (diabetic group without coronary artery disease) or with both diagnoses (combined group). We recorded the parameters of the most recent lipid analysis available, provided it had been performed within the 3 months preceding the inclusion of the patient or during the study visit. More details of the study design can be found in the original publication.5
The data of 6988 patients were analyzed. The mean age was 64.6 (11) years. There were 4382 men (62.7%). Of the 6988 patients in the overall group, 2586 (37%) belonged to the coronary group, 2654 (37%) to the diabetic group, and 1748 (25%) to the combined group. In all, 749 patients (9.7%) were excluded from the analysis. A group of 874 physicians participated: 437 (50%) were cardiologists; 201 (23%), endocrinologists; 166 (19%), internists; and 35 (4%), primary care physicians. The remaining 35 physicians (4%) were not classified.
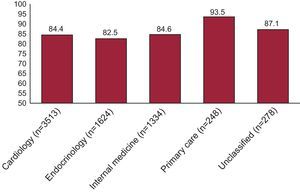
We studied the control of LDL-C concentrations according to the medical specialty. Figure 1 shows the percentage of patients whose LDL-C falls outside the recommended range. As can be observed, over 80% of the patients in all the participating specialties have LDL-C concentrations that surpass the recommended limits. The comparison of the proportions reveals a statistically significant difference (P<.001), a circumstance that could be related to a less widespread application of the guidelines in primary care.

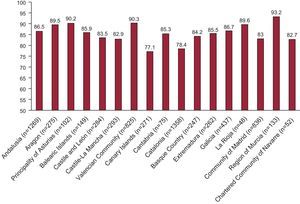
We also examined the LDL-C concentrations according to autonomous community. The percentage of patients who fall outside the recommended LDL-C range is shown in Figure 2. Over 80% of the patients are in this situation in all the communities except the Canary Islands (77.1%) and Catalonia (78.4%). The differences reached statistical significance (P<.001), a finding that may indicate that the clinical guidelines are more widely applied in those two communities.

These data show that the percentage of patients with adequate control of the LDL-C levels is insufficient, regardless of the specialty of the attending physician or where they live. This occurs despite the well-known fact that adequate control of cardiovascular risk factors in secondary prevention reduces the rates of morbidity and mortality. An important aspect of CODIMET is its contribution of data on a large population selected on the basis of high cardiovascular risk, consisting of patients with coronary heart disease or type 2 diabetes, considered to be the equivalent to cardiovascular disease. These data confirm the need to transmit and apply the recommendations of the clinical practice guidelines on a wider basis, especially taking into account groups of patients at high risk for experiencing cardiovascular events. The web page provides supplementary material offering additional data from the study.
These findings demonstrate that, in Spain, patients with very high cardiovascular risk, specifically patients with diabetes mellitus and/or coronary heart disease, very often do not achieve the recommended LDL-C levels, regardless of the specialty of the attending physician and the autonomous community in which they live.
FUNDINGThis study was financed by Merck Sharp & Dohme, MSD España.
CONFLICTS OF INTERESTGustavo Vitale and Belén González Timón are employees of Merck Sharp & Dohme, MSD España.
.