We present the case of a 50-year-old man (case 1) with hypertension and smoking habits, who presented with an ongoing chest pain for 2h and an ST-segment elevation on the antero-septal and lateral leads on the electrocardiogram, who underwent urgent cardiac catheterization.
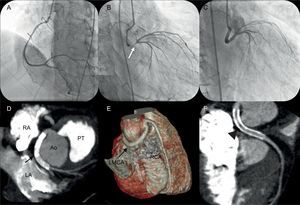
The coronary angiography revealed a dominant right coronary artery with no stenosis (Fig. 1A). The left main coronary artery (LMCA) was found to originate from the right coronary sinus, with a separate ostium from the right coronary artery and a retroaortic course. Severe lesions in the middle and distal-shafts of the LMCA were disclosed (Fig. 1B, white arrow). The anomalous LMCA was easily cannulated with a Judkins Left 4.0 catheter and successfully stented (Fig. 1C).

Acute pulmonary edema in the context of a hypertensive crisis, requiring mechanical ventilation, occurred in the immediate period after revascularization. Maximum troponin I levels were found to be 185.9μg/L. Recovery was uneventful and the left ventricular systolic function was only mildly compromised at discharge. Multislice computed tomography coronary angiography confirmed an LMCA retroaortic course (Figs. 1D and E, black arrows) and coronary stent patency (Fig. 1F, arrowhead).
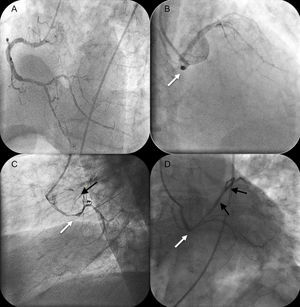
We also report the case of a 68-year-old man with hypertension, presented to the emergency department with ongoing chest pain. The electrocardiogram showed a left ventricular strain pattern with a left anterior fascicular hemiblock; the cardiac troponin I levels were found to be elevated (3.6μg/L) and the patient was admitted for a non-ST elevation acute myocardial infarction. The chest pain was refractory to maximum anti-ischemic therapy and urgent coronary angiography was performed. During cardiac catheterization, the patient's condition progressed to cardiogenic shock, requiring inotropic support and mechanical ventilation. The right coronary artery was a dominant vessel with a mild distal lesion (Fig. 2A), but the LMCA was arising from the right coronary sinus with a retroaortic course (Fig. 2B, white arrow). The LMCA had a middle-shaft severe stenosis (Fig. 2C, white arrow), and the left anterior descendent artery had a proximal critical lesion and was occluded at the middle segment (Fig. 2C, black arrow). LMCA cannulation was attempted without success with guiding catheters XB 3.5, Judkins Left 4.0, and Judkins Left 5.0. Finally, a multipurpose A1 catheter, allowed successful stent angioplasty of the anomalous LMCA and the left anterior descendent artery (Fig. 2D, white and black arrows). Hemodynamic improvement was immediate, allowing removal of inotropic support and mechanical ventilation within 24h. Recovery was uneventful and the patient was discharged with recovered left ventricle function. The patient did not cooperate to perform multislice computed tomography coronary angiography.

Most of the coronary anomalies are found incidentally in 0.6% to 1.3% coronary angiographies. Origin of the LMCA from the right coronary sinus is an extremely rare anomaly with an incidence of 0.017%.1
It is fundamental to identify the course of the anomalous LMCA: retroaortic, interarterial, septal, or anterior to the right ventricle free wall.1 Major prognostic relevance is attributed to the interarterial course of the LMCA, which is associated with sudden cardiac death, particularly during or immediately after strenuous physical exercise, as a result of coronary compression.2
The retroaortic course of the LMCA is a less frequent trajectory and is usually found to be benign,1 although it can seldom present with angina or even acute myocardial infarction.3 A multifactorial approach has been proposed to explain ischemia associated to the anomalous origin of the LMCA: slit-like coronary orifice with dynamic obstruction, acute angle take-off, or intramural segments of the anomalous coronary artery.3 However, in our cases, severe atherosclerotic coronary disease was disclosed, raising the hypothesis of an early atherosclerotic degeneration process, as seen in other coronaries with anomalous origin in the right coronary sinus, like the circumflex artery.4 In the RACES registry (a registry of 13 Spanish hospitals), atherosclerotic coronary disease (in any coronary) was found in association with 51% of patients5, although the true relationship between atherosclerotic coronary disease and coronary anomalies is unknown. In case 1, no additional atherosclerotic coronary disease was found and so, theoretically, an LMCA spasm could have been present.
Primary coronary angioplasty of an anomalous coronary artery is a challenging and highly complex intervention, particularly in the emergency setting. For a successful primary coronary angioplasty, it is fundamental to immediately and accurately recognize the anatomical details of the anomalous vessel.3
The retroaortic course of the LMCA, on coronary angiography, is identified by the visualization of the “dot sign”; it represents the artery visible at the end, posterior to the aortic root, on a 30° right anterior oblique incidence.6 However, the anomalous LMCA relation to the great vessels may be difficult to recognize because of the lack of a 3-dimensional visualization, only possible through multislice computed tomography coronary angiography.
This imaging technique can provide a more complete assessment of the origin, course, and anatomical relationship of the anomalous coronary with its neighboring structures, which is considerably relevant in the diagnosis and delineation of coronary intervention.2,3 It has the disadvantage of not being possible to perform in acute settings, as these require an emergency intervention.
A suitable selection of guide catheters, allowing a good coaxial alignment and backup support, is also essential for successful outcomes in anomalous LMCA angioplasty.3 Other types of guide catheters have been described previously3 and are selected on a case-by-case basis.
.