Keywords
INTRODUCTION
Despite technological progress, bifurcation lesions continue to present technical difficulties that are accentuated in certain anatomical conditions, such as extreme vessel tortuosity, extreme angulation of the origin of the side branch (SB) in relation to the main vessel (MV), or severe stenosis in both vessels, since they can prevent access and, as a result, treatment of the SB.1 In these situations, a steerable deflectabletip device may have a relevant role when dealing with this subgroup of lesions. We describe our experience with the Venture wire-control catheter (St. Jude Medical, Minnesota, United States) to cross the side branch in complex bifurcation lesions with an unfavorable anatomy in which conventional techniques had failed.
METHODS
Between April 2006 and September 2009, 553 patients with bifurcated lesions were treated percutaneously. We examined 20 (4%) patients in whom the Venture catheter was used when it was impossible to access the SB using conventional techniques and methods. Using a chronometer, we recorded the time taken to access the SB, and noted the number of guidewires used. The procedures were performed by an expert operator following a previously described stepwise strategy.2
We used the CardiOp-B system (Paeion, Rosh Ha'ayin, Israel) to measure the bifurcation angles: the take-off angle (between the proximal MV and the SB) and the carina angle (between the distal MV and the SB).3
Device and Procedure
The Venture catheter supports a 6 Fr guidewire catheter and is available in coaxial or monorail versions. The interior light makes it possible to use any coronary guidewire. It has a radiopaque 8-mm distal tip that can be deflected up to 90o with a clockwise torque shaft in the proximal area of the catheter. To avoid injury, the Venture catheter is advanced to the lesion in its straight configuration along a guidewire. Having reached the target, the tip is deflected to the desired angle. The fact that it can be deflected, together with the possibility of rotating the catheter tip in a circumferential plane, makes it easier to steer the guidewire and access the lesion, while providing excellent support. Once it has passed beyond the guidewire, it is turned anticlockwise to straighten the tip and thus can be withdrawn.4
We analyzed the success and complication rates of the Venture catheter, its influence on the number of guidewires used, and the duration of the procedure. Procedural was defined as succesful when the guidewire was passed through the true lumen of the SB allowing thus the further treatment of it with no complications. Serial determination of markers of myocardial damage (troponin, creatine phosphokinase [CPK], and the MB fraction of CPK) was performed.
Statistical Analysis
Quantitative variables are expressed as medians and 25-75 percentiles, and qualitative variables as percentages. Comparisons were made using a nonparametric test (Wilcoxon).
RESULTS
Baseline and Procedural Data
Table 1 shows clinical, angiographic and procedural data. At least, 2 guidewires were used before resorting to the Venture catheter (median, 3; 25-75 percentile, 2-3), whereas only 1 was needed with the Venture in the patients treated successfully (median, 1; percentile 25-75, 1-1) (P<.01) (Table 2). The median SB access time using conventional techniques was 16 minutes (25-75 percentile, 11.7-20.5), whereas this was reduced to 2.5 minutes (25-75 percentile, 1.8-3) using the Venture catheter (P<.01). Access times were reduced with experience in using the catheter, and this also influenced the success rate, since the failures occurred during the initial stages of the learning curve. In 10 (50%) patients, the catheter was initially used to access the SB; in 7 (35%) to cross the jailed side branch; and in 3 (15%), it was used in both stages.


Procedural Success
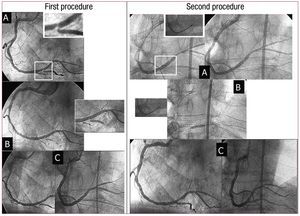
In 17 patients (85%), the guidewire was successfully used to access the SB and treat the bifurcation (Table 2). Figure 1 shows the first procedure in which this catheter was used. Only one complication occurred (patient 12) which was associated with a monorail catheter. This involved a patient with a severe lesion in the distal left main coronary artery. There was a severe, calcified and very angulated lesion at the origin of the circumflex artery, which required the use of the Venture catheter, following failure with various guidewires. Once the lesion was crossed, a guidewire was left as a marker and a stent implanted in the left main coronary artery, oriented toward the descending anterior artery covering the circumflex.

Figure 1. First procedure. A: severe lesion in the distal right coronary artery with a very angulated take-off of the posterior descending artery (PD). B: impossible to access the DP with a microcatheter and preformed guidewire. C: final result. Second procedure. A: Venture catheter. The deflectable tip allows the guidewire to be advanced. B: PD dilatation. C: final result.
For its subsequent dilatation, it was recrossed using the Venture monorail. When we attempted to withdraw the guidewire, it was partially torn, frayed, and wrapped around the catheter and the other coronary guidewires, making it impossible to extract it without removing the whole system, including the catheter. The procedure was finally completed successfully.
We did not observe any case of dissection or perforation, even though all patients had a severe lesion in the MV that left a very narrow lumen through which to direct the catheter. Figure 2 shows another example in which the Venture catheter played a key role in treating the bifurcation.

Figure 2. A: critical lesion in the left anterior descending/first diagonal. B: Venture deflected and guidewire advanced. C: Venture catheter. D: final result.
Hospital Outcomes
The majority of the patients (17/20; 85%) were discharged without complications. One patient with multivessel disease and ventricular dysfunction died after the procedure due to heart failure. Two patients developed a non-Q myocardial infarction due to the impossibility to recross jailed and compromised side branch despite using the Venture catheter.
DISCUSSION
Difficulties of Provisional Stenting
Currently, provisional stenting or a simple stenting strategy is the standard treatment for bifurcated lesions.5 Advancing a guidewire to the SB is a key maneuver for several reasons: it enables predilatation if required and, if it is occluded or dissected, it is useful as a marker of the true lumen. It also facilitates better intubation of the guidewire catheter when additional support is required. However, this can be difficult at times and we encountered problems in accessing the SB due to very severe lesions in both vessels or to an extreme angulation of the SB take-off. Furthermore, the stent in the MV may displace the carina and block the branch, which can complicate recrossing despite using a wide variety of coronary guidewires. Few studies describe the percentage of patients in whom it was impossible to access the SB. We previously reported a failure rate of 3%.6 It is in this group that the Venture catheter plays a role.
Another point of interest is that 6 patients had a 1.0.1 bifurcation.7 We think that this anatomy provides certain technical advantages, since the absence of disease in the distal segment of the MV allows better tip rotation and deflection, which facilitates orienting the guidewire toward the SB.
Previous Experience
Since McClure et al4 described the use of this catheter in a series of patients with complex coronary lesions, several authors have corroborated the safety and efficacy of this device.8-11 To date, this is the largest published series focused on the usefulness of the Venture catheter in bifurcation lesions, in which it was impossible to access the SB using conventional techniques. In these situations, the Venture catheter is the only tool that can steer the guidewire toward the lesion and that also provides additional support. Recently, Aranzulla et al11 have described the use of this catheter as an option after standard guidewires had failed in 18 patients with complex lesions (7 bifurcations), with an overall success rate between 78% and 85% in bifurcated lesions, similar to the values communicated by our group.
In terms of safety, complications associated with the catheter have not been documented. Our group experienced only one complication, described above, with the monorail catheter. This may have been due to the fact that the lateral opening of the catheter, which is slightly sharp, partially cut and frayed the guidewire during repeated rotation of the catheter.
In conclusion, the Venture catheter has been proven safe and effective and its use leads to successful outcomes in the percutaneous treatment of complex bifurcated lesions that would have failed using conventional techniques.
Correspondence: Dra. S. Ojeda.
Servicio de Cardiología. Hospital Universitario Reina Sofía. Avda. Menéndez Pidal, s/n. 14004 Córdoba. Spain.
E-mail: soledad.ojeda18@gmail.com
Received September 16, 2009.
Accepted for publication January 13, 2010.