Tropical endomyocardial fibrosis (EMF) is a largely unexplored condition that is endemic in tropical regions. EMF mainly affects people living in rural areas of low-income countries located in the jungles of the intertropical belt.1–3 Because of the lack of related systematic studies and limited access to health care of affected populations, the true prevalence of EMF is unknown. The disease is characterized by inflammation and fibrosis of the ventricular endocardium, which progresses to restrictive cardiomyopathy.3
The prevalence of EMF is highest in children and young adults.2 The pathogenesis of the condition is unknown, although several hypotheses refer to geographic, social, and nutritional factors, and a probable genetic susceptibility.1–3 The most widespread hypotheses cite exposure to parasites1,3 and a metabolic imbalance or toxicity due to a diet rich in tubers (especially cassava) and poor in proteins,1,3 with an excess of cyanide-releasing glycosides and deficient elimination of these compounds.
Here, we report the echocardiographic and clinical data (retrospectively collected between 2018 and 2021) of patients with EMF attending an urban hospital in Yaoundé, Cameroon, and 2 rural health centers, Obout and Bikop, located in the central region of the country in a jungle setting. The imaging studies were performed with QBit7 (Chison, China) and Vscan (General Electric, United States) ultrasound scanners. In 2 cases, ultrasound studies from other centers were recorded. The diagnosis was established based on reported criteria.2 Consent for inclusion was obtained from the patients, and the study was approved by the 3 participating centers.
Sixteen EMF patients were identified (1.05% of 1531 echocardiograms in total). The mean age of the patients was 23.5 years and mean age at diagnosis was 22.75 years, with 50% diagnosed in the pediatric age (7-15 years) and 75% before the age of 30 years. Twelve (75%) were males. All patients came from rural areas of the central region of Cameroon, were of low social status, and consumed protein-poor diets rich in cassava and other tubers. None of the patients were related.
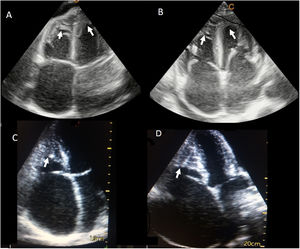
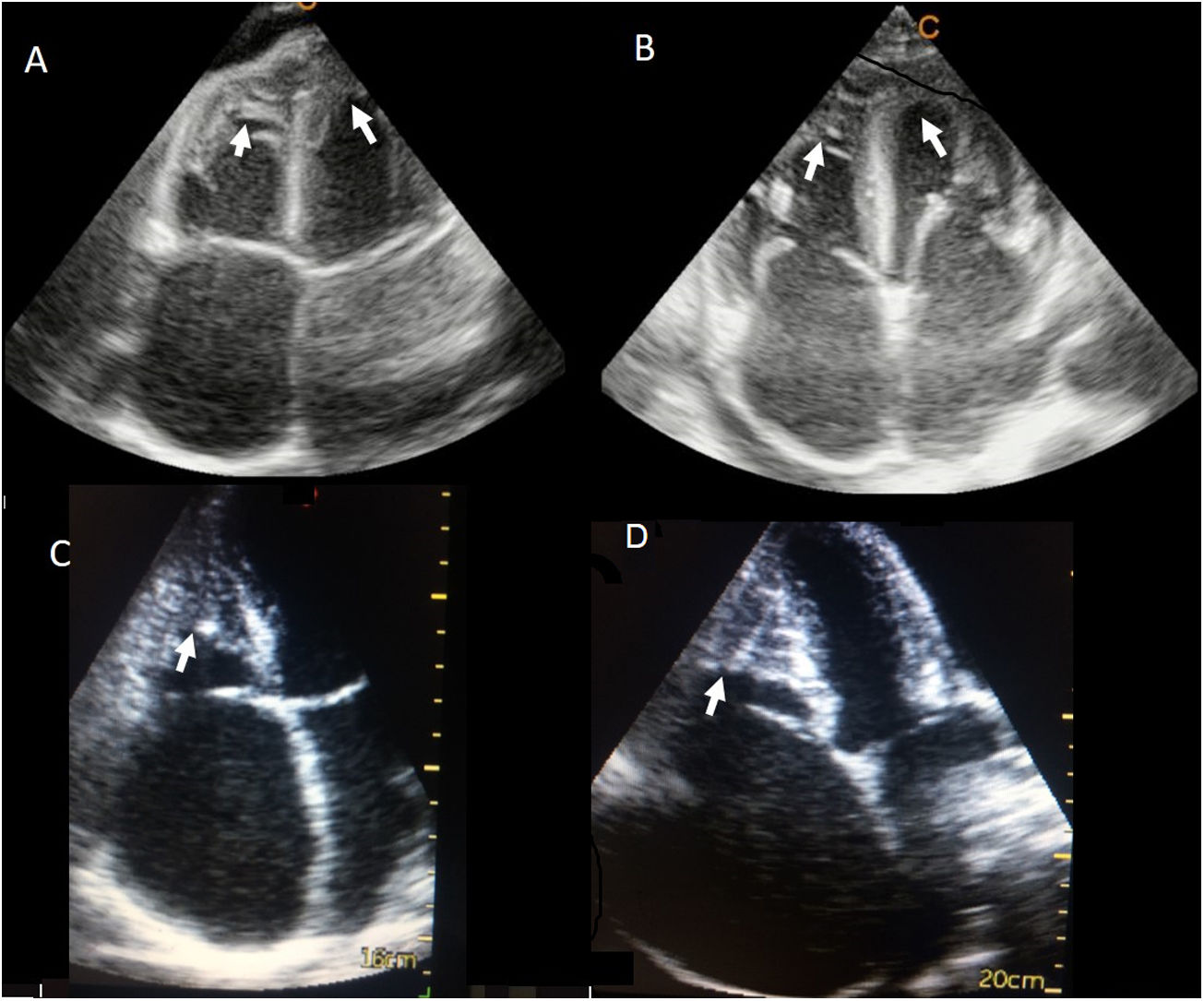
All those included had disease-related symptoms. Clinical data were available for 15 patients: 100% had dyspnea on exertion, 87% ascites, 60% lower limb edema, 40% facial edema, and 27% palpitations. The right ventricle (RV) alone was affected in 10 (62.5%) patients (mean age, 17.2 years) and both ventricles in 6 (37.5%) patients (mean age, 34.2 years) (figure 1). Analysis of the ventricular and valvular function of 2 patients was excluded, as they had severe pericardial effusion and ventricular collapse, which made this evaluation impossible. All patients had right atrial dilatation (severe in 86%) and RV dysfunction (severe in 43%). All those with biventricular involvement also had left atrial dilatation (severe in 71%). A single patient with moderate biventricular EMF had left ventricular dysfunction. Tricuspid regurgitation was observed in 100% of patients, and was severe in 64%. Mitral regurgitation was found in 71% of patients, severe in only 1. Tricuspid valve retraction (figure 1) was seen in 79%. In patients with biventricular EMF, 83% had mitral valve retraction. In all cases there was septal rebound and dilatation of the caval and suprahepatic veins. Pericardial effusion was present in 11 of the 16 patients (69%), and was severe in 4 (figure 2). Three patients had atrial fibrillation and the remainder showed sinus rhythm or tachycardia.
 and right ventricular (C and D) endomyocardial fibrosis. The arrows indicate the area of apical fibrosis. B: valve retraction is seen, due to adhesion of the subvalvular apparatus to the ventricular wall.")

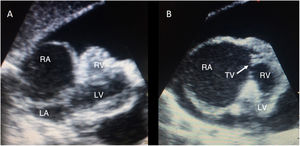
Ultrasound images of a patient with endomyocardial fibrosis and severe pericardial effusion, in the subcostal plane. A: conventional view: considerable RA dilatation, RV retraction, and compression of the left chambers. B: modified view centered on the right chambers. RA, right atrium; LA, left atrium; RV, right ventricle; LV, left ventricle; TV, tricuspid valve.
All patients received conventional medical treatment, but the symptoms persisted in all cases. Pericardiocentesis was required in 3 patients and paracentesis in 7. A complete blood count was available in only 3 patients; 2 of them showed eosinophilia.
Four patients died between 6 months and 7 years after symptom onset, and 3 were lost to follow-up. In the survivors, median follow-up since symptoms onset was 7 months (range, 2 months-15 years).
One patient was evacuated to Spain to undergo surgery, but he died before the procedure in right ventricular assist following progressive worsening. Magnetic resonance imaging confirmed the echocardiographic findings and showed evidence of multiple parasitosis.
EMF is an endemic disease with little-known characteristics. The single available screening study, performed in Mozambique, showed a much higher prevalence than is reported here—19.8% in endemic areas—and only 22.5% of patients had symptoms, which indicates substantial underdiagnosis.2 In keeping with the results of that study, we found a higher prevalence of the disease in males. The Mozambique study also identified a greater prevalence among cohabitants, which would support the hypothesis of diet as an etiological factor, an aspect that was not evaluated in the present study. A retrospective study4 in the pediatric population of Yaoundé, Cameroon, found EMF in 3.2% of patients with a diagnosis of heart disease. The socioeconomic data of the patients and their dietary profile were similar to those recorded here. Hypereosinophilia was detected in 61.4%. As in the present study, most patients had exclusively right heart involvement (79.6%). These data differ from those obtained in Mozambique, where 55% showed biventricular disease and only 28% exclusively RV involvement.2
Published survival data are scarce and from older studies (2-year mortality, 75%), although all research in this line indicates low treatment effectiveness and high mortality.1 There is some bias related to difficulties in accessing health care. Surgical treatment (endarterectomy, valve repair/replacement, and occasionally cavopulmonary bypass) improves the prognosis, but it may not be accessible, and the reported series are limited in number.1,3
The limitations of the present study are the small number of patients included and limited complementary studies performed.
In conclusion, EMF is a common, likely underdiagnosed disease in Cameroon that typically affects children and young adults from low-income, rural, jungle areas who consume protein-poor diets rich in cassava. Males show a higher prevalence and the RV alone is more commonly affected. EMF is characterized by a clinical syndrome of right heart failure with a high prevalence of ascites, even without peripheral edema, and a poor prognosis. Robust epidemiological population-based studies and prospective studies are needed to better understand the pathophysiology and course of this disease.
FUNDINGThis study received no funding.
AUTHORS’ CONTRIBUTIONSAll authors significantly contributed to the manuscript preparation and data collection. S. Cuenca: design, data analysis, and writing.
CONFLICTS OF INTERESTNone
ACKNOWLEDGEMENTSCentre Hospitalier Dominicain Saint Martin de Porres, Centre de Santé de Bikop and Centre Medical Christ-Roi d’Obout, Cameroon; Asociación Benéfica Doble Corazón, Malaga, Spain; Hospital Universitario Reina Sofía, Cordoba, Spain; Dr. Santiago José Ahumada, Hospital Costa del Sol, Marbella, Spain.